SMILE Eye Surgery Age Limits: When Is the Right Time for the Procedure?

If you are searching for SMILE eye surgery age limits, you are probably not just asking for a number. You are usually asking a more personal question: am I too early, too late, or at the wrong stage of life to do this well?
With Small Incision Lenticule Extraction (SMILE), the real question is not whether you have crossed a magic birthday but whether your eyes are at the right stage for a laser vision correction result to be worth it and to hold up well over time.
Age matters, but not in the way many patients assume. As an ophthalmologist and refractive surgeon, I do not treat this as a rulebook conversation. I treat it as a timing conversation within the broader context of refractive surgery and vision correction. This article walks through that timing question by life stage, so you can place yourself more clearly on the map.
Table of Contents
Why Age Feels Like Such a Loaded Question in SMILE Surgery
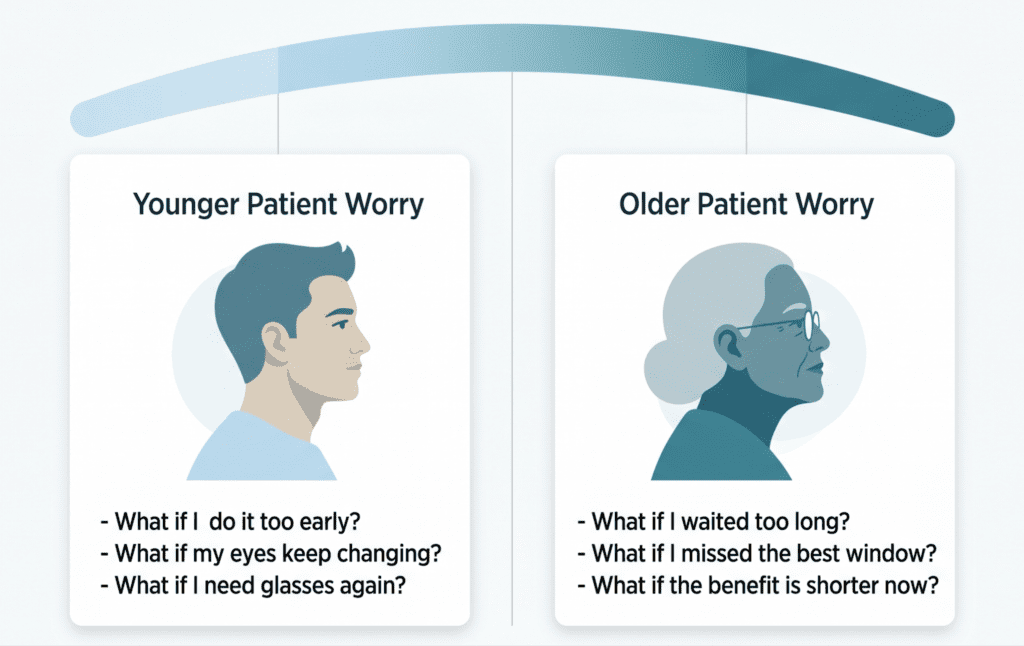
Patients usually come into this question from one of two directions. The younger version is: what if I do this too early, my eyes keep changing, and I end up needing glasses again? The older version is: what if I waited too long, missed the best window, and now the value of the procedure is lower than it would have been a few years ago?
Those are not vague emotional worries. They point to two real clinical issues.
On the younger side, the question is whether the prescription is truly stable. If the eyes are still changing, the timing may be wrong even if the patient is highly motivated and technically near the usual age range.
On the older side, the question is whether the lens inside the eye is starting to matter more than the cornea. Once presbyopia becomes part of the picture, the decision is no longer just about distance correction. It becomes a broader question about near vision, reading glasses, monovision, and whether a lens-based procedure deserves discussion.
That is why the age question feels so loaded. It is not really about a cutoff. It is about the right stage of life to do SMILE well and still feel good about the decision years from now.
Is There a Real Minimum Age for SMILE?
In the United States, the FDA-approved minimum age for SMILE is 22. If you are reading patient-facing information from U.S. clinics, that is the number you should expect to see first.
At the same time, many patients also see 18+ mentioned online and wonder why the numbers do not match. The reason is that some surgeons talk about off-label treatment in younger patients. Off-label does not automatically mean inappropriate or unsafe. It means the formal FDA indication is one thing and real-world surgical judgment can sometimes be broader.
Hitting 18 or 22 does not automatically mean you are ready. The number is only the beginning of the conversation. Prescription stability matters more.
Why Prescription Stability Matters More Than a Birthday
For younger patients, prescription stability is the central concept. When I say a prescription is stable, I do not mean it feels “mostly stable” or has changed only a little here and there. I mean there has been no meaningful trend of change over time. In practical terms, many surgeons think about stability as no more than about 0.50 diopters of meaningful change over 12 months, or about 1.00 diopter over 24 months. That matters whether the underlying refractive errors are mainly nearsightedness alone or nearsightedness with astigmatism.
That does not mean every tiny prescription tweak counts. This is where patients often get confused. A small shift in one direction one year and then a small shift back the other way is not the same as true progression. The bigger question is whether there is a trend. A surgeon is looking for directional change over time, not just isolated minor measurements.
This is why the phrase “mostly stable” is not always reassuring. A patient may have heard that their glasses prescription barely changed, but if the pattern still points in one direction, the eyes may not be truly settled yet.
Age is only a rough proxy for this. Some patients with low myopia may be genuinely stable at 19 or 20 years old. Others with higher prescriptions may still be changing at 24 or 25 years old. The important thing is not the birthday alone. It is whether the refractive change has actually stopped.
Your Early 20s: Why Some Patients Are Asked to Wait
When a patient in their early 20s is asked to wait, it is usually not because SMILE is inherently unsafe at that age. It is because the result may not hold as well if the eyes are still changing.
If surgery is done too early in a patient whose prescription is still progressing, the likely problem is that the eye keeps changing afterward. The patient may have excellent distance vision at first and then slowly drift away from that result over the next few years.
This is the real regret risk of doing it too early: the timing was premature, and the result may not hold as well as it ideally should.
At the same time, I would not present this as an argument for waiting unnecessarily. Once stability is clearly established, there is no built-in prize for postponing surgery for several more years. If a patient is truly stable, earlier treatment simply means more years of enjoying the benefit.
Mid-20s Through the 30s: Why This Is Often the Straightforward Window
For many patients, the mid-20s through the 30s is the simplest and most straightforward timing window for SMILE.
By then, prescriptions are often more settled. Presbyopia is usually not the dominant issue yet. The lens inside the eye is still not the main source of visual tradeoffs. In many cases, this makes the conversation cleaner: we are mostly talking about distance correction, clear vision, and whether the cornea and prescription are suitable.
That does not make this age range universal or automatic. I still look at stability, corneal topography, keratometry, ocular surface quality, overall eye health, the broader eye care picture, and patient expectations.
But if patients ask me which years are often the easiest from a timing standpoint, this is usually the range.
Your Late 30s and 40s: The “Did I Miss the Window?” Question
This is where the age conversation becomes more emotionally loaded.
Many patients in this stage are not worried that SMILE will stop working. They are worried they waited too long and are now about to spend money and effort on a procedure that may give them only a short period of uncomplicated benefit before reading glasses or other age-related changes reshape the picture.
If you are in your late 30s or 40s, the question is no longer just whether SMILE can still improve your distance vision. In many cases, it can. The more useful question is whether distance correction alone is still the right plan, or whether near vision, monovision, or a lens-based option now deserves more attention.
Presbyopia, Readers, and Monovision
The reason this conversation changes is presbyopia.
Presbyopia is the normal age-related loss of near focusing ability that usually starts becoming noticeable in the 40s. It happens because the natural lens inside the eye becomes less flexible over time. SMILE works on the cornea. It does not stop the lens from aging.
This is one of the most important things older patients need to understand: SMILE can still improve distance vision, but it does not prevent the need for reading glasses later. If you want the fuller discussion of what that settled distance vision can feel like, SMILE Eye Surgery Results covers that separately.
That is why monovision starts coming up in this age range. Monovision means correcting one eye primarily for distance and the other for nearer work. For some patients, this can be a very practical compromise. For others, it feels unnatural and they dislike it quickly.
The key point is that monovision should not be guessed at. I usually want to simulate it first with a contact lens trial. The patient lives with that setup for a few days, drives, works, reads, uses screens, and does normal daily activities. Some people know almost immediately that they cannot tolerate it. Others adapt well, but still need a little time to feel sure. That trial can be extremely helpful before making a permanent surgical decision.
When the Lens Starts to Matter More Than the Cornea
At some point, especially in the mid-to-late 40s and beyond, the aging lens can become the bigger issue than the cornea. This is the point where refractive lens exchange (RLE), rather than a corneal procedure like SMILE, may start to make more sense.
That shift needs to be explained clearly, because it is not a contradiction. It is a different decision that solves a different problem.
SMILE is a corneal distance-vision procedure. RLE is a lens-based procedure. It is more involved, more expensive, and carries more risk because it involves removing the natural lens and placing an intraocular lens. But it can also address the fact that near and intermediate vision are now becoming major parts of the complaint, and it removes the need for cataract surgery later on.
That does not mean every patient in their late 40s or early 50s should move straight to RLE. Some patients still mainly want better distance vision now, are comfortable wearing over-the-counter reading glasses, and do perfectly well choosing SMILE or another corneal approach. The important point is that by this age, the conversation is no longer only about whether SMILE can work. It is about whether it is still the best category of solution.
If you want the fuller discussion of how the procedure itself works, SMILE Eye Surgery Basics covers that separately.
What Matters More Than Age Alone
If I had to redirect a patient away from age obsession and toward the things that matter more, I would emphasize prescription stability, corneal shape and thickness, ocular surface quality, lens status, and realistic expectations.
Age is useful, but mostly because it points us toward these deeper questions.
In younger patients, age raises the question of stability. In older patients, age raises the question of presbyopia and lens aging. In both directions, the number is acting more like a signal than a verdict.
Common Myths About SMILE Surgery Age Limits
One common myth is: “If I am 18 or 22, I am automatically ready.”
That is not true. You may have reached a number and still not be stable enough.
Another is: “If I am over 40, it is too late.”
That is also not true. Many patients over 40 can still improve their distance vision meaningfully. The real issue is whether they are willing to accept the near-vision tradeoffs or whether a lens-based strategy would make more sense.
Another is: “SMILE will stop future vision changes.”
It will not. It can correct your current distance prescription. It does not stop presbyopia. It does not freeze the natural aging of the lens. It does not guarantee that your eyes will never change again.
The Best Questions to Ask at a SMILE Consultation
If you are unsure whether this is the right time, these are the questions I would want you to bring:
- Is my prescription truly stable, and over what time period are you judging that?
- Do my old records show a trend or just small noise?
- If I am in my 40s, what are my likely near-vision tradeoffs?
- Is monovision worth trialing in my case?
- Is corneal surgery still the right category for me, or is the lens becoming the bigger issue?
- If now is not the best time, what would you want to see change before moving forward?
Those questions are more useful than asking for a perfect age.
What to Remember About SMILE Surgery Age Limits
There is no single perfect age for SMILE, and there is no one number that answers the timing question by itself. The lower-age conversation is really about stability. The older-age conversation is really about presbyopia, lens status, and what kind of visual strategy makes the most sense now.
If this is not the right time, that does not usually mean the door has closed. It usually means the timing or the procedure choice needs to be better matched to where your eyes are now. A good consultation should help you understand that clearly, without urgency and without false reassurance.
Frequently Asked Questions About SMILE Surgery Age Limits
What is the minimum age for SMILE eye surgery?
In the United States, the FDA-approved minimum age is 22. However, the more clinically important question is whether the prescription has truly stabilized and whether the patient is a good fit for this type of refractive surgery.
Can I get SMILE at 18?
Some surgeons may discuss treatment in younger patients off-label, which is one reason 18+ appears online. But turning 18 does not automatically mean the timing is good. The real question is whether the prescription has stopped meaningfully changing.
Is there an upper age limit for SMILE?
There is not a single hard upper age cutoff in the same way there is a lower-age conversation. The bigger issue is that in the 40s and beyond, presbyopia and lens aging start changing which procedure may make the most sense.
Can I get SMILE at 40?
Yes, many patients can. The real question is not whether 40 years old is “too old.” It is whether you mainly want distance correction and accept that reading glasses may still become part of the picture, or whether a lens-based strategy deserves discussion.
What does a stable prescription mean for SMILE candidacy?
It means there has been no meaningful trend of change over time. A common practical way to think about it is no more than about 0.50 diopters of meaningful change over 12 months, or about 1.00 diopter over 24 months.
Will SMILE stop my prescription from changing?
No. SMILE corrects your current distance prescription. It does not stop presbyopia, and it does not freeze the natural aging of the eye or guarantee that your prescription will never change again.
What is monovision, and how do I know if it is right for me?
Monovision means correcting one eye more for distance and the other more for near work. It can work well for some patients, but not for everyone. That is why many surgeons first test it with a contact lens trial before making a surgical decision.
Do conditions like dry eye, glaucoma, or keratoconus change the age conversation?
Yes. Age alone never decides candidacy. Dry eye symptoms, glaucoma, suspicious topography, or keratoconus can all affect whether the timing is right or whether SMILE procedure is the best option at all. This is also why the age question should never be separated from the rest of the eye health picture.
How is this different from SMILE eye surgery from LASIK?
The age and stability logic is broadly similar in LASIK eye surgery and SMILE: the key issues are still prescription stability, corneal suitability, and life stage. The procedural differences, including the fact that LASIK involves a corneal flap while SMILE does not, matter for other discussions, but they do not replace the basic timing question.
If SMILE is not the best fit, what other options might come up?
Depending on the case, a surgeon may discuss LASIK, PRK, or a lens-based option instead. That is especially true if the main issue is not your age by itself, but your corneal shape, refractive range, or longer-term visual priorities.