Punctal Eye Plugs for Dry Eye Treatment: A Clinical Guide to Who Benefits and Why
When patients hear they might benefit from punctal plugs, the reaction is almost always the same: you’re putting something in my eye? It’s understandable. The name sounds clinical, and the idea of a procedure anywhere near your eye can feel daunting before you understand what it actually involves.
The reality is far simpler than most people expect. A punctal plug, also known as a lacrimal plug, sits at the opening of the tiny drainage canal on the inner edge of your eyelid, not on the eye itself. Think of it like a small earplug for your tear drain. There’s already a natural opening there, and the plug simply rests at its entrance to slow how quickly tears drain away from the surface of your eye.
Nothing gets placed in the eye — the plug goes in the eyelid, in the drainage canal. It’s far less invasive than it sounds, and for most patients, the procedure takes just a few minutes. Any awareness of it fades within moments of leaving the chair.
The other misconception we often encounter is that punctal plugs are a last resort — something to consider only after every drop, supplement, and lifestyle change has been exhausted. In practice, the opposite is often true. Punctal plugs, particularly collagen plugs, dissolve naturally and carry virtually no risk. They can be one of the earliest and most practical tools in a dry eye treatment plan.
For patients who are busy, prone to forgetting drops, spending long hours on screens, or wearing contact lenses, plugs can offer real, consistent relief with very little effort on their part. Punctal Plugs, in my view, are one of the best first steps in dry eye treatment simply because the risk is low and patients respond well. There is genuinely no reason to wait.
In this article, I explain how punctal plugs work, who benefits most from tear retention, when they are less effective, how different materials compare, what the procedure actually feels like, and how to decide whether they belong in your dry eye treatment plan.
Table of Contents
Understanding Your Tear Drainage System
Your tear system is a continuous, dynamic cycle. It’s not a reservoir. Every time you blink, your lacrimal glands release tears onto the surface of the eye, spreading a protective film across the cornea. Your meibomian glands, which line the edges of your eyelids, contribute an oily layer that slows evaporation.
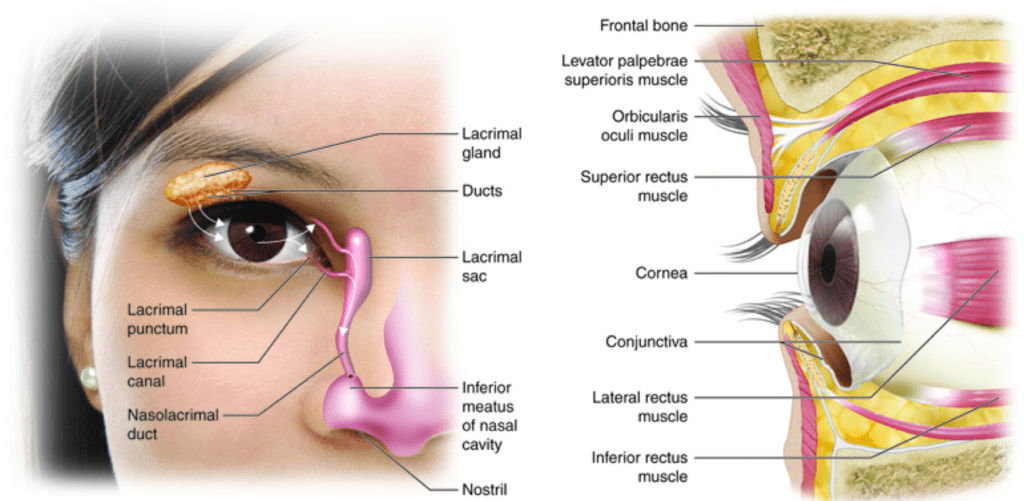
Image credit: Colorado Community College
When tears have done their job, they drain through two small openings on the inner corners of your upper and lower eyelids called the puncta, through a channel called the canaliculus, into the lacrimal sac, and eventually down into the nose and throat. This is why eye drops sometimes leave a faint taste at the back of your throat.
What punctal plugs do is straightforward: they partially block the puncta at the corner of your eye, so natural tears spend more time on the surface of the eye.
It’s important to understand, though, that plugs don’t improve tear quality. If there’s underlying inflammation or your meibomian glands aren’t producing adequate oil, plugs alone won’t resolve that.
Plugs give the tears that your tear ducts generate a better chance of staying where they’re needed. For patients whose drops work well but wear off too quickly, that extra time on the surface makes a real difference. For mild dry eye, it can sometimes be enough on its own with minimal side effects when properly selected and placed.
Not All Dry Eye Is the Same
One of the most important things I want patients to understand is that dry eye is not a single eye condition. It’s an umbrella term for several different problems, and the treatment that helps one patient may do very little for another. Getting the diagnosis right is what makes the difference.
There are two primary types:
- Aqueous-deficient dry eye: the eye isn’t producing enough tears.
- Evaporative dry eye: the more common of the two, where tears disappear from the surface too quickly, usually because the meibomian glands aren’t producing sufficient oil to keep them there.
Most patients have both components to some degree, which is why treatment rarely involves just one approach.
Because punctal plugs work by keeping tears on the surface longer, they are most useful when there are actually tears worth retaining. For patients with a mixed evaporative and aqueous component — which is the majority — plugs are genuinely helpful because slowing drainage gives the tear film more time to do its job before it breaks down.
Even in patients whose tear quality isn’t ideal, retaining whatever moisture is present still provides meaningful relief.
Where plugs tend to be less effective is in patients whose dry eye is driven almost entirely by meibomian gland dysfunction with very little aqueous component, or in patients with active ocular surface inflammation.
In those cases, you’re either retaining a tear film that’s already compromised by poor oil quality or potentially keeping inflammatory mediators on the surface longer than you’d want. That’s why ophthalmologists always assess and address inflammation before or alongside plug placement, not instead of it.
There’s also a subset of patients whose symptoms of dry eye far outpace their clinical signs. They report significant discomfort, but the ocular surface examination doesn’t reflect that level of disease. In these cases, the pain is often driven by hypersensitive corneal nerves rather than true tear deficiency, and plugs are unlikely to provide the relief they’re hoping for. Recognizing this early saves patients from a procedure that won’t address the real problem.
Where Punctal Plugs Fit in a Dry Eye Treatment Plan
Punctal plugs are not a standalone cure for dry eye. They are one tool within a broader treatment plan. By the time most patients visit us, they have already tried artificial tears with limited or inconsistent relief. We typically begin with four things working in parallel:
- Punctal plugs
- Over-the-counter lubrication,
- Lid hygiene, and
- Inflammation control through prescription drops (cyclosporine, lifitegrast, or loteprednol)
Each addresses a different part of the problem, and they work better together than any single one does alone.
The question patients ask most often is when to treat inflammation versus when to place plugs. The answer depends on what the ocular surface looks like.
If the tear film is heavily laden with debris or the lid margin is significantly compromised, it makes sense to treat the surface first and revisit plugs once things have stabilized. More often, both issues are present simultaneously, and addressing them in parallel is both safe and more efficient.
Plugs rarely worsen symptoms. In the worst case, they simply don’t help. When sequencing does matter, it’s usually because placing plugs in the presence of significant untreated blepharitis or active inflammation means retaining a tear film that is already working against the ocular surface rather than for it.
Patients who view plugs as a last resort should understand that a punctal plug is a reversible, in-office procedure that takes minutes, requires no recovery, and is covered by insurance. The barrier to trying it is low. The potential benefit is real. There is no clinical reason to save it as a last resort.
Temporary vs. Long-Term Plugs: What Changes
Broadly speaking, there are two types of punctal plug categories: temporary and longer-term. The difference is not simply how long they last, but how they behave inside the drainage system and how they are tolerated over time.
Collagen Plugs: The Low-Risk Entry Point
Collagen plugs are temporary. They dissolve naturally over weeks to months, depending on the formulation. Because they sit within the canal rather than protruding above it, they are rarely felt once in place.
In my practice, collagen plugs are extremely predictable. They do not cause irritation, they do not cause infection, and they do not migrate in a way that creates problems. If they dislodge, it happens early, not months later.
For that reason, I often begin here. They allow us to test how much benefit tear retention provides without committing to a long-term device. If symptoms improve with a temporary plug, that confirms tear retention is contributing to relief.
Lack of immediate relief, however, does not necessarily mean punctal occlusion will not help long-term. In some cases, surface inflammation or gland dysfunction still needs to be addressed before the full benefit becomes apparent.
If symptoms do not improve even after those factors are controlled, it tells us we need to look more closely at tear quality, gland function, or the possibility of a neuropathic component.
Silicone Punctal Plugs: Durable, But Not Always Ideal
Silicone plugs are designed for longer retention. They can remain in place for extended periods and provide sustained tear preservation. However, they sit at the punctal opening and can sometimes rub against the surrounding tissue.
In rare cases, they can become associated with inflammation or infection. While uncommon, I have seen significant reactions that required oral antibiotics and close monitoring. Another practical issue is that if a silicone plug falls out and the patient does not notice, symptoms may return and be interpreted as treatment failure rather than device loss.
For these reasons, I am selective about when I use long-term silicone plugs. They are effective, but they are not always the first choice.
Hyaluronic Acid: A Custom Alternative
There is another option that is discussed far less often: injectable hyaluronic acid placed into the punctum. This semi-permanent plug (gel) conforms to the patient’s own canal anatomy and typically lasts around six months.
Because it molds to the natural shape of the drainage system, it avoids some of the mechanical irritation associated with rigid devices. For patients who repeatedly lose plugs or who are sensitive to silicone, this can be an excellent alternative.
Permanent Closure: When We Know It Works
In select patients, especially those with clear evaporative components who respond strongly to temporary plugs and are tired of repeat visits, permanent punctal cauterization can be considered.
This involves numbing the area and closing the punctal opening with controlled cautery. It is a definitive solution, but it is only appropriate when we are confident that tear retention is consistently beneficial. I rarely move directly to a permanent treatment option without first confirming a response.
Material and Design Differences in Puntal Plugs
| Feature | Collagen (Temporary) Plugs | Silicone (Long-Term) Plugs | Hyaluronic Acid Gel |
| Duration | Dissolve naturally over weeks to months | Designed to remain long-term | Typically lasts ~6 months |
| Positioning | Sit fully within the canal | Often includes a cap that rests at the punctal opening | Injected into the canal; conforms to anatomy |
| Visibility | Not visible once placed | Cap may be visible at the surface | Not visible |
| Foreign Body Awareness | Rare once seated properly | Possible if the cap rubs against the conjunctiva | Rare |
| Infection / Inflammation Risk | Extremely low in clinical experience | Low but higher than collagen; rare serious reactions possible | Very low; biologically compatible material |
| Risk of Falling Out | Uncommon; if dislodged, usually early | Can fall out over time without patient noticing | Uncommon due to molding effect |
| Biofilm Risk | Minimal due to dissolution | Theoretical risk over time with permanent material | Minimal |
| Best Use Case | Early intervention, low-risk trial, compliance support | Select long-term cases when tolerance confirmed | Patients with repeated plug loss or sensitivity to silicone |
| Reversibility | Dissolves naturally | Removable in-office with gentle micro-forceps under topical anesthesia | Gradually resorbs |
What Punctal Plug Insertion Feels Like: Awareness, Anxiety, When to Be Concerned
In a punctal plug insertion, the anticipation is almost always worse than the procedure itself. The first time can feel nerve-wracking simply because it involves the eye, but once patients experience it, that anxiety usually disappears.
When we perform an insertion, we numb the surface of the eye with topical anesthetic drops. Patients may feel gentle pressure or slight touch during insertion, but not pain. The entire process takes only a few minutes.
Immediate Sensation After Placement
Right after insertion, some patients report being aware that something was done. That awareness typically fades within a minute or two. It is important to distinguish between procedural awareness and true irritation.
With collagen plugs placed correctly inside the canal, there is no exposed material rubbing against tissue. Once positioned, there is essentially nothing to feel. If a patient describes a persistent sensation, I examine the plug to confirm placement. If it is seated properly within the canal and not protruding, there is no anatomical reason for ongoing mechanical irritation.
Silicone plugs are different. Because some designs include a small cap at the punctal opening, patients may be intermittently aware of them, particularly during blinking. That sensation should not be painful. If it is, the position needs to be reassessed.
Psychological vs Mechanical Awareness
There is also a psychological component. Some patients remain focused on the idea that something is there. If proper positioning is confirmed and any mechanical causes are ruled out, persistent awareness is rarely due to pathology. It is more often heightened attention to the area. Removing a properly seated plug for psychological awareness does not address the underlying dry eye problem.
When Sensation Is Not Normal
True warning signs are uncommon but clear:
- Persistent pain rather than mild awareness
- Redness that worsens rather than improves
- Discharge or swelling
- Excessive tearing/watery eyes, or irritation that does not settle
Those situations warrant reassessment. In most cases, however, once the initial procedure is complete and the eye has settled, patients return to normal activity without restriction and stop noticing the plug entirely. The most common feedback I hear at follow-up is simple: “I forgot it was even there.”
Why Some Patients Feel No Relief Even When the Plug Is Positioned Correctly
A properly placed punctal plug does exactly what it is designed to do: it slows tear drainage. If a patient feels no improvement, the issue is not the plug itself but the underlying biology. The most common reason is incomplete treatment of meibomian gland dysfunction.
Dry eye is not purely aqueous-deficient or purely evaporative. Most patients have a combination. If the oil layer is unstable and evaporates quickly, simply retaining tears is not enough. The tear film still breaks up too soon. In those cases, plugs need to be paired with gland treatment and inflammation control.
Another factor is active ocular surface inflammation. If the tear film contains significant inflammatory mediators, retaining it without treating the inflammation first may not provide relief.
That is why I assess the quality of the tear film and the lid margins carefully before or alongside plug placement. Sometimes we treat the surface first and place plugs after stabilization. More often, we manage both at the same time.
True worsening is rare. If plugs do not help, they are usually insufficient on their own.
There is also an entirely different category of patient: those whose symptoms far exceed their clinical signs. The surface looks relatively quiet, yet the discomfort is significant. In these cases, the problem is hypersensitive corneal nerves rather than tear deficiency. In such cases, the focus should shift toward therapies that address nerve-related pain instead of tear retention.
When punctal plugs are used in the right patient, and as part of a broader strategy that includes lubrication, gland care, and inflammation control, they provide meaningful improvement. When they fail, the explanation is usually diagnostic, not mechanical.
Plug Fallout, Migration, and What It Actually Means
One of the most common concerns patients have is: what if the plug falls out?
In reality, plug loss is uncommon, particularly with collagen plugs. If a collagen plug dislodges, it almost always happens early, not months later.
Silicone plugs can fall out over time, especially if the punctum is large or the sizing is slightly off. When that happens, patients may not notice the loss immediately. Symptoms return, and it can appear as though the treatment stopped working.
When Fallout Is Meaningful
While a single plug loss is not alarming, repeated plug losses suggest something about the anatomy. The punctal opening may be unusually narrow, irregular, or shaped in a way that does not retain standard devices well.
Lid mechanics can also play a role. In those cases, we reassess the approach. Options such as hyaluronic acid gel, which conforms to the canal, may be more appropriate.
Migration and “Lost” Plugs
Patients sometimes worry that a plug can migrate deeper into the drainage system and cause harm. With properly sized and positioned plugs, significant migration is rare. Collagen plugs dissolve. Silicone plugs are designed to sit at the punctal opening with a retaining cap.
True internal migration requiring intervention is uncommon. If a patient reports new discomfort, tearing, or swelling, we evaluate it. But in routine practice, meaningful migration events are not something I see frequently.
Infection, Biofilm, and Safety: What Is the Real Risk?
Whenever we place any device in the body, the question of infection naturally comes up. That concern is reasonable. In routine practice, infection related to punctal plugs is uncommon. The risk depends largely on the material used.
Collagen plugs dissolve naturally and are biologically compatible; the rate of infection or significant inflammatory reaction is extremely low. Because they resorb over time, they do not create a persistent foreign surface where bacteria can accumulate. For that reason, they are a very safe starting point.
Silicone plugs remain in place long-term, and any permanent foreign material carries a theoretical risk of biofilm formation. While serious complications are rare, they are more likely with silicone than with dissolvable plugs.
I have seen significant inflammatory reactions associated with silicone plugs. These are not common, but when they occur, they can require oral antibiotics and close monitoring. In very rare cases, more aggressive treatment may be necessary.
This difference in risk profile is one reason I am selective about long-term silicone placement.
When to Delay or Avoid Placement
There are situations where it makes sense to pause before placing plugs.
If a patient has active conjunctivitis, significant blepharitis, or uncontrolled ocular surface inflammation, I prefer to stabilize the surface first. Retaining tears that contain inflammatory debris does not improve comfort.
Once the surface is controlled, plugs can be placed safely.
Special Populations: Who Benefits From Punctal Plugs
Punctal plugs are not reserved for a narrow subset of patients. When used thoughtfully, they serve multiple roles: stabilizing the ocular surface before surgery, supporting autoimmune disease, improving contact lens tolerance, and reducing the burden of daily drop use.
| Patient Group | Why Punctal Plugs Help | Key Clinical Insight |
| Sjögren’s / Autoimmune Dry Eye | Tears evaporate rapidly; retaining even limited moisture improves surface stability | Retention becomes foundational, not optional |
| Pre-Refractive Surgery (LASIK, SMILE) | Stabilizes tear film before measurements; improves postoperative comfort | Surface optimization improves refractive accuracy |
| Pre-Cataract Surgery | Stabilizes the tear film before biometry, reducing variability in intraocular lens calculations | Prevents measurement variability and refractive surprises |
| Contact Lens Wearers | Reduces midday dryness and drop dependency | Improves lens tolerance with minimal effort |
| Elderly Patients With Dexterity Issues | Decreases reliance on frequent drop instillation | Improves treatment consistency |
| Busy Screen-Heavy Professionals | Provides continuous support without requiring frequent drops | Practical compliance solution |
| Mixed / Unstable Dry Eye | Enhances baseline tear retention when combined with gland and inflammation treatment | Works best as part of layered therapy |
| Anatomical Considerations (Lid Laxity, Canal Shape) | Effectiveness is influenced by eyelid mechanics and punctal anatomy | Proper sizing and assessment matter |
The key is not the category alone, but how punctal occlusion fits into the overall treatment strategy for that individual patient.
Cost, Coverage, and Long-Term Maintenance
One of the practical questions patients ask is whether punctal plugs are considered elective. They are not.
Punctal plug placement is a medical treatment for dry eye disease and is generally covered by insurance, including Medicare and most private plans. As with any medical service, deductibles and individual coverage details vary, but this is not viewed as a cosmetic or optional procedure.
What Ongoing Maintenance Looks Like
The maintenance depends on the type of plug used. Collagen plugs dissolve over time. If they are effective, they may need to be replaced every few months. The replacement visit is brief and straightforward, but it does require periodic follow-up.
Longer-term options reduce the frequency of visits, but they carry different considerations, including tolerance and material selection. Some patients ultimately choose permanent cauterization once we have confirmed consistent benefit from temporary plugs and are confident that tear retention is clearly helpful.
How to Decide if Punctal Plugs Are Worth Trying
The decision to place punctal plugs is based on objective findings and symptom patterns. The decision depends on tear film behavior, eye health at the surface, and whether tear retention addresses the underlying mechanism of symptoms.
The framework below outlines how I evaluate whether plugs are likely to help.
| Step | What to Evaluate | Clinical Implication |
| Step-1 | Do artificial tears help, but wear off quickly? | – Yes → Tear retention likely beneficial- No → Symptoms may not be drainage-related |
| Step-2 | Assess tear film stability (tear breakup time or TBUT) | – Short TBUT → Slowing drainage may improve surface stability |
| Step-3 | Evaluate ocular surface inflammation | – Significant debris/inflammation → Treat surface first- Controlled surface → Safe to proceed |
| Step-4 | Identify evaporative component (MGD) | – Mixed aqueous + evaporative → Plugs useful with gland treatment- Pure MGD with minimal aqueous → Plugs alone unlikely to suffice |
| Step-5 | Screen for neuropathic pain pattern | – Severe symptoms with minimal clinical signs → Consider nerve-driven pain; plugs unlikely to resolve core issue |
| Step-6 | Consider practical factors | – Autoimmune dry eye (e.g., Sjögren’s)- Contact lens intolerance- Preparing for refractive/cataract surgery- Difficulty using drops consistently |
| Step-7 | Weigh risk–benefit profile | – In-office, topical anesthesia- No incisions, no downtime- Reversible- Generally insurance-covered- Low complication rate when properly selected |
If the clinical signals align and inflammation is controlled, temporary punctal plugs represent a low-risk, practical next step.
In Summary
Punctal plugs are not a cure for dry eye but a mechanical tool used in modern eye care to improve tear retention. When an eye doctor determines that tear drainage is contributing to symptoms, and plugs are placed at the right time alongside gland care and inflammation control, they can provide meaningful, measurable benefit with minimal risk.