Bladeless LASIK Surgery Guide: What I Want Patients to Understand Before They Decide

Most patients who come to me asking about bladeless LASIK procedure are really asking something bigger. They want to know whether LASIK is safe, whether it will hold long-term, and whether the version they read about online is actually what a careful surgeon would recommend for their eyes.
Those are the right questions to start with.
The phrase “bladeless LASIK” comes from traditional LASIK procedure where flap creation was performed using a mechanical microkeratome (a blade-based device) rather than a laser. With the changes in LASIK technology, LASIK surgeons today use a state-of-the-art femtosecond laser for that step, making the term “bladeless” largely irrelevant. But the more useful question to ask is not whether LASIK is bladeless but whether LASIK is the right procedure for your particular eye.
This guide walks through what modern all-laser LASIK eye surgery involves, what the procedure feels like, how candidacy is evaluated, and when I would recommend SMILE or EVO ICL instead. I have had LASIK myself, and I have performed refractive surgery for staff members in my own practice. That context shapes how I counsel patients, as a framework for making a decision they will be comfortable with long term.
Table of Contents
Understanding the Fear That Surrounds LASIK
The fear around LASIK is not abstract. Patients usually come in worried about a few very specific things:
- something touching the eye
- losing control during surgery
- panicking in the middle of the procedure
- risk of complication they cannot undo
By the time many patients see me, they have already read online stories about chronic dry eye, halos, glare, depression, and regret. I do not think those fears should be brushed aside. LASIK is elective. It permanently changes the cornea. Patients are not irrational for worrying about those outcomes, and they deserve clear, honest counseling.
It also helps to say this plainly: pre-surgery anxiety around LASIK is extremely common. I have had LASIK myself, so I remember what it feels like to be on the patient side of the conversation. I have also performed refractive surgery for employees and staff members in my own office. I mention that because I would not make those decisions lightly.
Believing in LASIK does not mean recommending it for everyone. Good refractive surgery depends on selecting the right patients and recommending the right procedure.
That discussion starts with understanding how modern LASIK works, because many patients are still using terminology from an older era of refractive surgery.
How Modern LASIK Works
To understand LASIK, it helps to start with the cornea, the clear front surface of the eye. The cornea does a large part of the eye’s focusing. In refractive errors such as myopia, hyperopia, and astigmatism, light is not being focused on the retina as precisely as it should be.
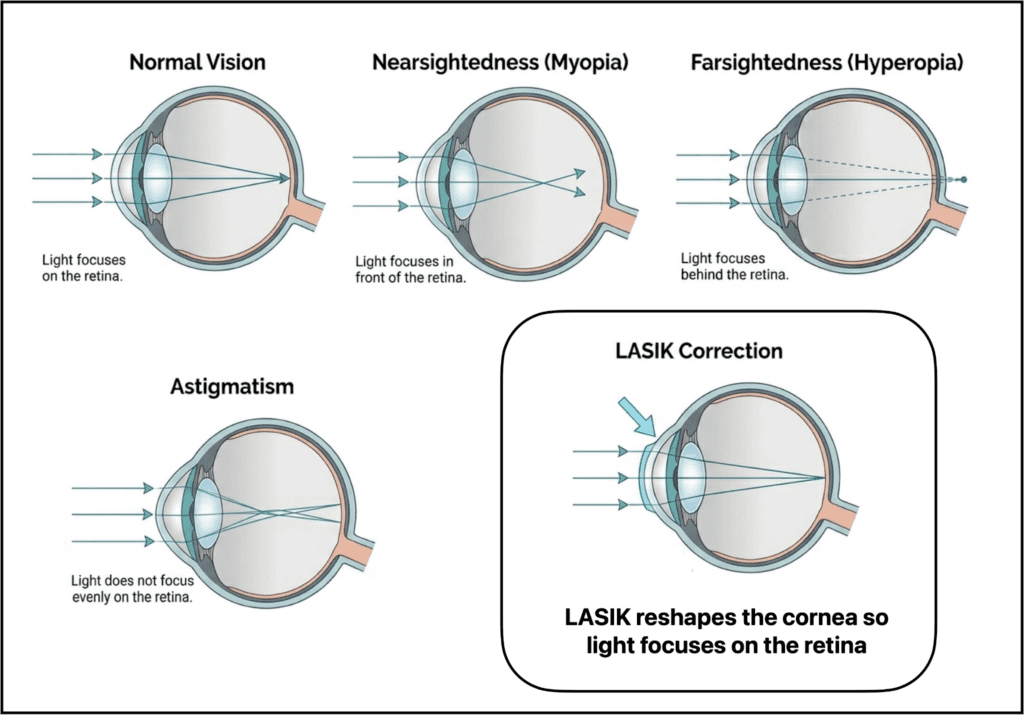
LASIK works by changing the shape of the cornea so that light focuses more accurately. That reshaping is extremely small and highly controlled.
In myopia, the central cornea is typically flattened slightly. In hyperopia, the treatment pattern is designed to steepen the center. In astigmatism, the laser smooths out asymmetry in the way the cornea bends light.
Patients do not need to remember those optical details, but it helps to understand the basic idea: LASIK does not place a lens in the eye or work deep inside the eye. It reshapes the cornea, which is the front window of the eye.
Modern LASIK has two main steps:
First, we create a very thin flap in the cornea. This is the part patients sometimes still call “bladeless LASIK,” because modern LASIK uses a femtosecond laser for flap creation rather than the older mechanical microkeratome.
Next, we lift that flap to reach the corneal layer underneath, where the excimer laser does the corneal reshaping.
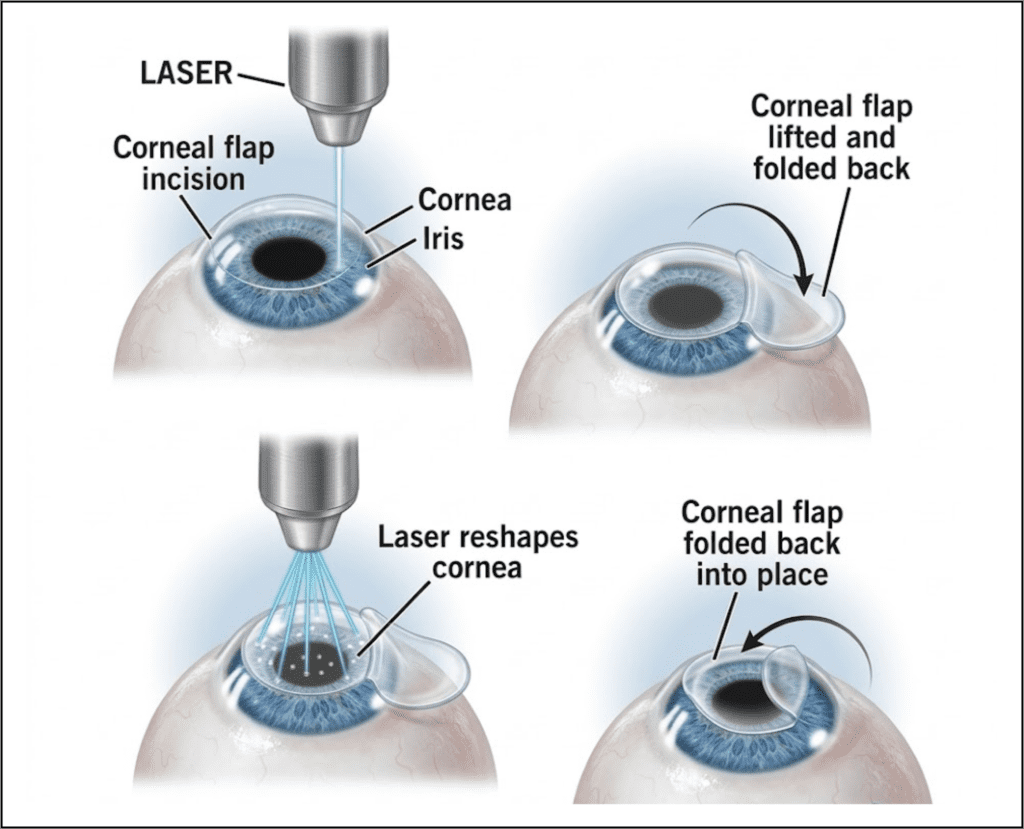
The excimer laser does not cut in the ordinary sense of the word. It removes microscopic amounts of corneal tissue according to a treatment plan that is based on the patient’s measurements. Once that reshaping is complete, we place the flap back into position. It acts like a natural bandage while the eye heals, which is one reason LASIK recovery is generally faster and more comfortable than surface procedures such as PRK.
For anxious patients, one detail is often especially reassuring: LASIK is performed on the cornea, not inside the eyeball. The treatment is happening on the front surface of the eye, and it is guided by detailed pre-operative measurements. That does not make it casual or risk-free, but it does make the surgical procedure much easier to understand than many patients imagine before they see it explained clearly.
The shift from microkeratome flap creation, which used a mechanical blade-based device to create the corneal flap, to femtosecond flap creation improved precision and predictability. Today, the discussion centers on candidacy, corneal safety, dry eye, treatment planning, and whether LASIK is the right procedure in the first place.
What Happens on the Day of Surgery
On the day of surgery, your eye is numbed with eye drops and a lid speculum is placed so you do not have to worry about blinking. The flap is created first, then lifted, the excimer laser treatment is performed, and the flap is repositioned. There are no stitches.
The treatment itself is brief. In many modern LASIK cases, the full procedure is over in about 10 minutes. The flap-creation step may last only seconds. With a modern femtosecond laser platform such as the VisuMax 800, that part may take around 9 seconds. On older femtosecond platforms, it may take closer to 20 to 30 seconds.
While the advanced technology and the speed is reassuring, it should not be confused with casual treatment. The outcome still depends heavily on the screening, measurements, corneal imaging, tear-film evaluation, and treatment planning that happened before the patient ever lies down under the laser.
Preparing Patients Before LASIK Surgery
Many LASIK articles jump from candidacy straight into the laser room. In real life, preparation matters. Before I treat anyone, I want stable measurements.
That usually means:
- contact lenses need to be stopped ahead of time so the cornea can return to its natural shape before measurements are taken
- soft lenses are typically stopped for at least a week or two before final measurements, while rigid gas permeable lenses often require a much longer break
I also want the ocular surface optimized before I trust the numbers. If the tear film is unstable, the measurements are less reliable. That is one reason dry eye has to be taken seriously before surgery.
On the day of the procedure itself, patients are advised to come in without eye makeup, heavy lotions, or creams around the lids. They will also need someone to drive them home afterward.
These small practical details matter. They reduce avoidable stress on a day when patients are already mentally loaded.
What It Feels Like Under the LASIK Laser
Patients often expect me to talk first about pain. However, with modern LASIK, patients generally do not feel sharp pain because the eye is numbed. What they notice instead is pressure, touch around the lids from the speculum, fluid sensation, lights, blurred vision, and the awareness that something is happening while I am talking them through it.
The experience can also vary depending on the platform being used. With a modern femtosecond laser platform such as the VisuMax 800, the flap creation experience can feel different from older femtosecond systems. Patients may notice the touch of the interface, a fluid sensation, a green fixation light, and some blur during that step, but not the same pressure-heavy feeling or temporary blackout that older systems were known for.
During the excimer portion, I ask patients to look toward the fixation light while the laser reshapes the cornea. Vision is blurry during that phase. That is normal and expected. What helps most is narrating each step as we go. Patients tend to do better when they know what they are feeling and why.
What Happens If You Panic or Move During LASIK
This is one of the first fears anxious patients bring up, and rightly so. The fear is usually that even a small eye movement will throw the laser off target and cause something to go wrong.
Modern LASIK systems are designed to account for small eye movements. Fixation targets, eyelid stabilization, and excimer eye-tracking systems all help keep the treatment aligned properly.
That does not mean patient cooperation does not matter. It does. Patients still need to listen, focus, and stay reasonably calm. But ordinary anxiety is common, and the procedure is planned with that in mind. Continuous guidance during surgery patients know what is coming next. If someone is especially anxious, that can be addressed beforehand with counseling and, when appropriate, anxiety-relieving medication.
It is also worth mentioning that an elective procedure such as LASIK does not need to be rushed. If a ou feel too overwhelmed to move forward, taking more time, asking more questions, or seeking a second opinion can be a sensible part of the decision-making process.
Is Modern LASIK Actually Safer?
Compared with older microkeratome LASIK, femtosecond-flap LASIK improved the precision and consistency of flap creation. In a large retrospective case series of 81,238 LASIK procedures, early flap displacement was reported in 0.003% of femtosecond cases compared with 0.033% of microkeratome cases, which is roughly a ten-fold lower rate with femtosecond flap creation (Clare et al.).
But even with this high success rate, I do not like presenting LASIK safety as a simple yes-or-no verdict based on one laser technology label. The most important safety issue is still selection. A well-chosen patient with a healthy cornea, stable measurements, and a properly managed tear film is in a very different category from a patient who should have been steered toward SMILE, ICL, or no surgery at all.
The more useful discussion is whether the cornea is actually a good LASIK cornea, whether topography or tomography looks reassuring, whether the dry eye workup is being taken seriously, and whether another procedure would fit better.
Who I Consider a Good LASIK Candidate
A good LASIK candidate is identified by a combination of factors rather than one isolated measurement. A strong candidate usually has:
- a stable prescription
- healthy corneal shape and adequate corneal thickness
- no signs of keratoconus or early ectatic change
- a manageable ocular surface without severe untreated dry eye
- expectations that match what LASIK can and cannot do
Expectations matter more than many patients expect. Wanting LASIK is not the same thing as being a good candidate for it. LASIK can reduce dependence on glasses or contacts for distance vision, but it does not stop the rest of the eye from aging. It does not prevent presbyopia. It does not prevent future cataracts. It does not promise that the healing process will feel effortless.
When I Recommend Something Other Than LASIK
This is where clinical judgment matters most, because LASIK is not automatically the best fit for every eye.
SMILE
For many patients with straightforward myopia, or nearsightedness, SMILE deserves a serious discussion. It is a laser vision correction metod that does not involve a flap. It preserves more corneal integrity and can reduce some of the flap-related concerns that make patients uneasy. In the right patient, it may also reduce the dry-eye burden compared with LASIK.
LASIK still has important strengths. It may be favored when there is a need for the flexibility of topography-guided treatment, when the patient has hyperopia, or when the refractive pattern makes LASIK the more precise option.
PRK
PRK is the procedure patients often assume must be the conservative fallback. In practice, that is usually not how it is approached. PRK is almost never preferred over LASIK when a patient is already a good LASIK candidate. Its recovery is longer and often much more uncomfortable.
The narrow situations where PRK enters the discussion are edge cases, such as certain irregular astigmatism scenarios where the patient is not a good LASIK candidate and the refractive numbers do not qualify well for ICL. In rare situations, PRK may even be paired with cross-linking on the same day.
EVO ICL
For patients whose corneas are not ideal for laser reshaping, EVO ICL may be the better vision correction surgery, especially in high prescriptions or eyes with thin cornea where preserving corneal tissue and visual quality is the priority.
Recovery After LASIK Surgery
Post-operative eye care for LASIK is minimal in terms of lifestyle disruption and pain, with most patients returning to work and normal activities within 24–48 hours. While most patients experience minimal discomfort, one should not expect perfection on day one. During the recovery time, the first several hours after LASIK, it is normal to experience:
- burning, tearing, or scratchiness
- light sensitivity
- hazy or filmy vision
- fluctuating clarity
By the next day, many patients already see dramatically better, but the eye surface is still healing. Dryness, glare, halos, starbursts, and visual fluctuation can still occur in the first week and first month while the tear film and cornea stabilize.
These symptoms are often part of early healing and improve over time, but they can affect driving, confidence, and quality of life while they are present.
Pupil size, corneal shape, treatment design, and proper patient selection also influence how likely these visual symptoms are to occur. When the pre-operative workup is thoughtful and the treatment plan fits the eye, the odds of troublesome night-vision symptoms are low.
The key is not simply noticing any symptom at all, but recognizing a pattern that is worsening rather than settling.
Severe pain, a clear drop in vision, increasing redness, discharge, or concern that the flap may have been disturbed should prompt a call right away. Those changes suggest that the eye should be examined rather than simply watched at home.
Dry Eye After LASIK: Why Prevention Matters
LASIK can temporarily worsen dryness because the procedure affects the cornea and can disrupt tear-film stability during healing. Patients who already have meaningful ocular surface disease are at higher risk of struggling after surgery if that issue is not identified in advance.
That is why prevention matters before LASIK. The tear film should be optimized before final measurements are taken. Punctal plugs may be used proactively for some LASIK patients, and selected patients may benefit from anti-inflammatory therapy such as cyclosporine ahead of surgery. Attention to meibomian gland function, lid hygiene, and the overall quality of the tear film also matters, because if the surface is poor, both comfort and measurement accuracy suffer.
The more useful clinical question is whether the ocular surface is being evaluated and treated carefully enough before surgery, because that affects both the quality of the treatment plan and the comfort of recovery.
Questions to Ask Your Surgeon Before LASIK
A good LASIK consultation should leave room for direct questions. Some of the most useful ones are:
- How are you screening me for dry eye?
- What features of my cornea would make you advise against LASIK?
- Why are you recommending LASIK instead of SMILE, PRK, or ICL?
- Which risks are most relevant to my specific eyes and prescription?
- In what situation would you tell a patient not to have surgery?
These questions help shift the discussion toward candidacy, planning, and whether LASIK is the right procedure for that particular eye.
Long-Term Results After LASIK
While LASIK permanently reshapes the cornea, it does not mean vision can never change again. The rest of the eye continues to age and may need vision correction. The lens can stiffen, causing presbyopia. Cataracts can develop later in life. Some patients, especially those who started with higher prescriptions, may have some refractive drift over time.
None of that means the corneal treatment itself reversed. Our guide to LASIK permanence and longevity discusses long-term stability in more detail.
A LASIK flap is also a permanent anatomical change to the cornea. In normal daily life, a healed flap is generally very stable, but it does not mean the eye has returned to an untouched state. If an enhancement is ever needed later, the right answer depends on why the vision changed, what the cornea looks like at that point, and whether another corneal procedure still makes sense.
How to Choose a Refractive Surgeon
Credentials matter, but the consultation matters just as much. When a refractive evaluation is being done well, it should include:
- a careful refraction and full ocular exam
- corneal imaging that evaluates shape and structural risk
- a serious dry-eye assessment
- a discussion of alternatives, not just LASIK
- realistic expectation-setting about benefits, limitations, and side effects
Patients should also be wary of clinics that can offer only one answer. If a surgeon performs LASIK, SMILE, PRK, and ICL, that surgeon is in a much better position to recommend what fits the patient rather than what fits the menu.
Continuity matters too. The eye surgeon should be involved in the pre-operative evaluation, the procedure itself, and the follow-up. Elective laser eye surgery should not feel fragmented.
Is LASIK Worth It?
Modern bladeless LASIK eye surgery is a legitimate, well-studied procedure. Whether it is the right choice depends on the specific patient, not the procedure in the abstract.
Some patients are excellent LASIK candidates and do very well. Others are better served by SMILE, ICL, or simply waiting until the prescription is more stable. A smaller group will hear from me that surgery is not the right answer at all.
Long-term contact lens wear is also not as neutral as it feels. Patients who rely on contacts for years can develop keratitis, chronic irritation, inflammation, and blood vessel growth at the corneal periphery, sometimes even with careful lens hygiene. I raise that not to push patients toward surgery, but because an honest comparison should run in both directions.
Whatever brings a patient to this conversation, the decision at the end of it should come down to one thing: whether this particular eye is genuinely a good fit for the procedure being recommended, and whether the surgeon in front of them is willing to say so either way.
Frequently Asked Questions
Is bladeless LASIK painful?
Most patients do not feel pain during LASIK because the eye is numbed beforehand. You may notice pressure, the touch of the speculum, and fluid sensation, but sharp pain is not a typical part of the experience.
What happens if I move my eye during LASIK surgery?
Modern LASIK systems are designed to account for small eye movements. Fixation targets, eyelid stabilization, and tracking systems keep the treatment aligned. Normal involuntary movement during surgery does not typically cause a problem.
How long does LASIK surgery take?
The treatment itself takes about 10 minutes per eye. Femtosecond flap creation can take as little as 9 seconds on newer platforms. The full visit is longer due to preparation, instructions, and post-operative checks.
What are the most common recovery symptoms after LASIK?
Dry eye, temporary light sensitivity, halos, and glare during healing are the most common. Most improve as the cornea stabilizes over the first weeks to months. Serious complications are rare with careful patient selection and screening.
Who is not a good candidate for LASIK?
Patients with unstable prescriptions, thin or irregularly shaped corneas, severe dry eye, or very high refractive errors may not be good LASIK candidates. In many of these cases, SMILE or EVO ICL may be a better fit.