Astigmatism can be frustrating because the vision is often not simply “blurry.” Patients describe blurred or distorted vision, ghosting, halos, shadowing around letters, a slight doubling effect, or vision that is almost clear but not quite sharp. Some notice that their contacts blur after blinking, or that squinting helps temporarily. Others report night vision problems, or find that a new pair of glasses makes the floor look tilted or changes their depth perception.
Those symptoms do not automatically mean something is wrong with the eye. In many patients, regular astigmatism is a refractive error, meaning the eye is not focusing light cleanly on the retina. The eye needs correction in a specific amount and in a specific direction. When that correction is accurate, stable, and comfortable, glasses, contact lenses, or other prescription lenses can often give clear, reliable vision.
The harder part is that astigmatism correction is more sensitive than a simple myopia or hyperopia prescription. Eyeglasses, toric contact lenses, daily disposable torics, rigid gas permeable lenses, hybrid lenses, and scleral lenses all correct astigmatism differently. The best option depends on the prescription, the eye surface, the way the lens fits, the patient’s lifestyle, and how stable the vision needs to be.
This guide explains how astigmatism corrective lenses work, why toric contacts sometimes blur or rotate, when glasses may be the better choice, and when specialty lenses should be considered.
Table of Contents
Why Astigmatism Corrective Lenses Feel Different
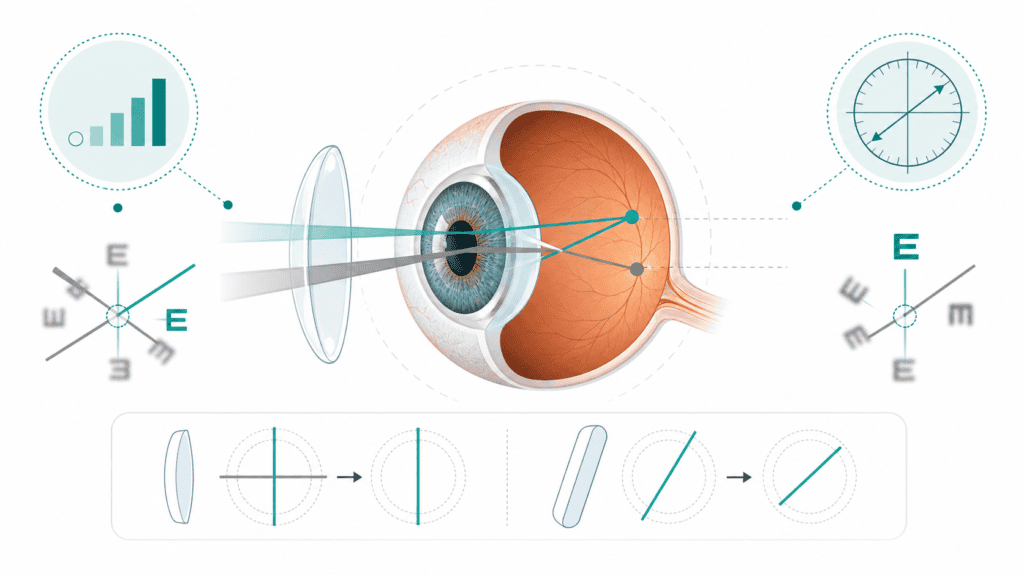
Astigmatism correction feels different because it is directional. A simple prescription changes focusing power overall. Astigmatism correction has to correct uneven focusing in a particular meridian.
That is why a patient may feel that the vision is sharp in one way but distorted in another. Letters may look shadowed. Headlights may look smeared. A contact lens may seem clear for a moment and then blur after a blink. A new glasses prescription may make vision clearer but also feel strange for several days.
Regular astigmatism is not a disease or a personal failure. It is a measurable part of the prescription. Glasses and contacts do not cure astigmatism permanently, but they can correct it while the lenses are being worn.
Symptoms can also overlap with dry eye. If vision changes through the day, worsens with screen use, or improves briefly after blinking or using lubricating drops, the tear film may be part of the problem. That does not replace the need for the right astigmatism prescription, but it can affect how stable the correction feels.
Cylinder and Axis: The Amount and the Direction
Two numbers matter most in an astigmatism prescription: cylinder and axis.
Cylinder is the amount of astigmatism correction and may be written as “cyl” on a prescription. Like other forms of lens power, it is measured in diopters. Axis is the direction where that correction is placed. A useful way to think about it: “the amount and the direction.” Both have to be right for the correction to feel natural.
This is also why small prescription changes can feel more noticeable with astigmatism than patients expect. If the cylinder is stronger, the axis usually needs to be more precise. A small axis change may be barely noticeable in one patient and very noticeable in another, depending on the prescription and how sensitive the visual system is to the change.
Patients do not need to memorize the optical details. The practical point is simpler: astigmatism correction is not just about making the prescription stronger or weaker. It is about placing the correction accurately.
How Glasses Correct Astigmatism
Glasses correct astigmatism by placing cylindrical power at the correct axis in front of the eye. Because the lenses are fixed in the frame, glasses can provide very stable correction. They do not rotate on the eye the way a contact lens can.
That stability is one of the main advantages of glasses. They may be especially useful for patients with dry eye, contact lens intolerance, higher astigmatism, complex prescriptions, or jobs where contacts are difficult to manage. Patients who also have presbyopia may need the prescription to account for reading vision — through reading glasses, progressives, or another near-vision solution — in addition to the astigmatism correction.
Glasses are also important even for patients who prefer contacts. Every contact lens wearer should have backup glasses. That is not because contact lenses are inherently unsafe. Contacts can be safe and effective when they are fitted well and worn properly. But the eye still needs rest days, and patients need an alternative if a lens tears, irritation develops, an infection is suspected, or the doctor recommends stopping contact lens wear temporarily.
Backup glasses are part of responsible contact lens care, not a sign that contacts have failed.
What to Expect When Adjusting to New Astigmatism Glasses
New astigmatism glasses can feel strange at first, especially if this is the first time cylinder correction has been added or if the axis has changed meaningfully.
Patients may notice:
- peripheral distortion
- a tilted-floor sensation
- mild nausea
- altered depth perception
- vision that is sharper but feels “off”
- discomfort when switching between old and new glasses
Those symptoms do not always mean the prescription is wrong. The brain may need time to adapt to the new directional correction. In some cases, especially when the prescription change is large, the doctor may prescribe the correction in a stepwise way rather than giving the full change all at once.
That said, patients should not force themselves through symptoms that feel unsafe. If the glasses cause persistent distortion, headaches, eye strain, difficulty walking, or vision that does not settle after a reasonable adaptation period, the prescription and the glasses should be checked. The issue may involve the cylinder amount, the axis, the frame fit, the lens placement, or the way the new correction was introduced.
Regular Contacts vs. Toric Contacts
Regular soft contact lenses mainly correct spherical power, such as myopia or hyperopia. Toric contact lenses add astigmatism correction.
The difference is that toric contacts need to sit in the correct orientation on the eye. A regular soft lens can rotate without affecting vision much. A toric lens has directional correction, so if it rotates too much or settles inconsistently, the vision may blur or fluctuate.
This does not mean contacts cannot correct astigmatism. Many patients with regular astigmatism do very well in toric contacts. The lens design, fit, material, and stabilization all matter.
There is also some nuance. Very mild astigmatism may not always require a toric lens if the patient sees comfortably in a regular spherical contact. On the other hand, a patient with more noticeable cylinder may feel that regular contacts leave a shadow or ghost image that glasses correct more clearly.
Glasses and contact lens prescriptions also do not always feel identical. A contact lens sits directly on the eye, while glasses sit in front of the eye. The doctor may need to adjust the contact lens prescription, lens brand, or fit to get the best balance of clarity and comfort.
Why Toric Contacts Can Blur, Rotate, or Feel Unstable
When toric contacts work well, they can give clear and comfortable vision. When they do not, patients often feel stuck in a cycle of “almost clear” vision.
Common reasons toric contacts blur or feel unstable include:
- lens rotation or poor alignment
- a fit that is too loose or otherwise unstable
- diameter or base curve mismatch
- dry eye or tear-film instability
- reduced blinking during screen use
- deposits or buildup on reusable lenses
- lens material that does not work well with the patient’s eye
- stabilization design that does not settle well
- prescription or axis mismatch
- a normal adaptation period with a new lens
The timing of the blur can give the doctor useful clues. Blur that happens right after blinking may point toward lens movement or fit. Vision that gets worse later in the day may involve dryness, deposits, buildup, or the eye’s tolerance for contact lens wear.
This is not something patients should have to diagnose themselves. During a contact lens evaluation, the clinician may check how the lens moves, where it settles, whether it rotates, how the tear film looks, whether deposits are present, and whether the cylinder and axis need adjustment.
Daily Disposable Toric Contacts: Cleaner and Healthier When Available
Daily disposable toric contacts can be helpful because they remove many cleaning and deposit variables. The patient starts with a fresh lens each day and discards it at night.
That can matter for patients whose reusable lenses become blurry later in the day, collect buildup, feel less comfortable with wear time, or create hygiene concerns. Because contact lenses sit directly on the eye, the doctor is always thinking about comfort, oxygen, cleanliness, and long-term corneal health.
When the prescription is available and the cost is practical, daily disposable torics are often preferable. But they are not available for every astigmatism prescription, and they are not automatically the right answer for every patient. Some prescriptions require reusable soft lenses, custom soft torics, rigid gas permeable lenses, hybrid lenses, or scleral lenses.
Reusable lenses are not automatically unsafe. They simply require a different level of care and consistency.
Dry Eye, Screens, and Blurry Contact Lenses
Dry eye can make astigmatism correction feel unstable. Even if the prescription is correct, an uneven tear film can scatter light and make vision fluctuate.
This often becomes more noticeable during screen use. When people concentrate on a screen, they tend to blink less completely and less often. For a contact lens wearer, that can make the lens feel drier and the vision less consistent, especially late in the day.
Practical steps may include:
- using rewetting drops if recommended
- taking breaks during prolonged screen work
- keeping the screen slightly below eye level
- checking whether the contact lens fit or material is contributing
- considering daily disposables when appropriate
- wearing glasses for part of the day when the eye needs a break
Persistent dryness, burning, redness, or blur should be evaluated rather than repeatedly self-managed. In some patients, dry eye treatment has to be part of making astigmatism correction work well. For patients who need more support for the tear film, Manhattan Eye also has a guide to punctal plugs for dry eye.
When Glasses May Be Better Than Contacts
Glasses are not a fallback. For many patients, they are the most stable and predictable astigmatism correction.
Glasses may be the better option when:
- the patient wants the most stable vision
- dry eye makes contact lenses uncomfortable
- toric contacts repeatedly rotate or blur
- the patient has contact lens intolerance
- the astigmatism is higher or more complex
- hygiene or handling is difficult
- the work environment makes contacts less practical
- the patient wants lower maintenance
Some patients wear contacts for sports, social situations, or certain workdays and use glasses the rest of the time. That mixed approach is often very reasonable. The goal is not to prove that one option is superior in every situation. The goal is to match the correction to the eye and the patient’s life.
When Soft Toric Contacts Work Well
Soft toric contacts often work well for mild to moderate regular astigmatism when the prescription is stable, the tear film is healthy, and the lens fits predictably.
They can be especially useful for patients who dislike wearing glasses during exercise, work, photography, social events, or daily activities where frames feel inconvenient. They can also be very satisfying when the first fitting is approached with realistic expectations.
The first toric lens tried is not always the final best lens. Brand, material, lens movement, stabilization design, comfort, and axis alignment can all affect the result. A patient may need more than one trial lens before the fit and vision feel right.
That fitting process is normal. It does not mean toric contacts “do not work.” It means the lens has to match the eye.
When to Consider RGP, Hybrid, or Scleral Lenses
Specialty contact lenses may be worth considering when standard soft toric lenses do not provide stable clarity or comfort. They may also be considered for higher astigmatism, irregular astigmatism, suspected keratoconus or other corneal irregularity, significant dry eye, or patients who want the sharpest optical quality possible.
It is important not to think of specialty lenses only as a last resort for severe disease. Rigid gas permeable and scleral lenses can sometimes improve visual quality even in regular astigmatism because the optics are different from soft lenses.
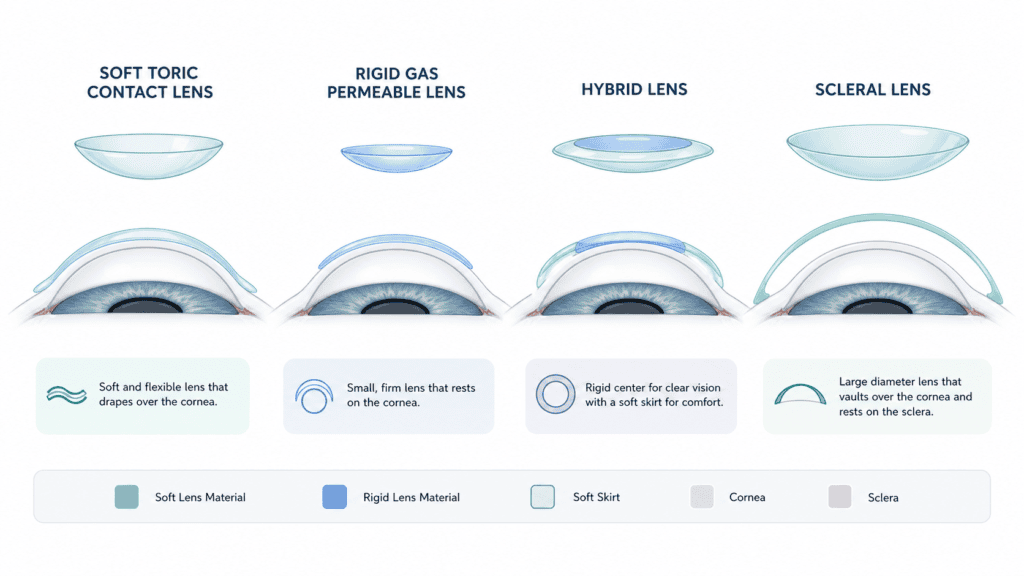
The main specialty lens categories are:
- RGP lenses: smaller rigid contact lenses that can provide crisp optics and help neutralize astigmatism.
- Hybrid lenses: lenses with a rigid center and a soft skirt.
- Scleral lenses: larger rigid lenses that rest on the white of the eye and vault over the cornea, which can help both vision and dryness in selected patients.
These lenses require more specialized fitting. They may involve multiple visits, a learning curve for insertion and removal, and a higher upfront cost.
The day-to-day routine is also different from disposable soft lenses. RGP and scleral lenses are custom devices that are cleaned, stored, and reused. Patients do not replace them every day or every few weeks the way they might with disposable soft contacts. That means the cost, maintenance routine, and follow-up visits can be different.
Needing a specialty lens does not automatically mean the eye is damaged. It means the eye may need a more customized optical solution.
What About Overnight Reshaping Lenses?
Orthokeratology, often called Ortho-K, uses specially designed rigid lenses worn overnight to temporarily reshape the cornea. The temporary change in corneal shape allows some patients to go without glasses or contacts during the day.
Patients interested in Ortho-K should ask whether their prescription and corneal profile make them a candidate. For most patients with astigmatism, the primary corrective lens choices are glasses, soft toric contacts, daily disposable torics, custom soft lenses, RGP lenses, hybrid lenses, or scleral lenses.
Contact Lens Availability, Cost, and Insurance
Astigmatism contact lens choices are partly limited by what is manufactured in the patient’s prescription. Product ranges change, so it is not useful to make rigid claims about exactly which powers are available in which lens. But the general principle is consistent: some astigmatism prescriptions and lens power combinations have many options, while others have fewer.
Very low cylinder powers may not be available in some lens lines. Higher astigmatism may have fewer daily disposable options. Some patients need monthly lenses, custom soft torics, RGP lenses, hybrid lenses, or scleral lenses.
Cost and insurance can also differ widely by lens type. Standard soft toric contacts are often treated as a routine vision expense or an out-of-pocket purchase. Specialty custom lenses may sometimes qualify for medical insurance coverage when there is medical necessity, such as irregular astigmatism, keratoconus, or certain corneal conditions. Coverage depends on the diagnosis and the insurance plan.
Useful questions to ask before committing to a lens plan include:
- Is the fitting fee separate from the lens cost?
- How often will the lenses need to be replaced?
- Is this considered a routine vision benefit or a medical lens benefit?
- Are follow-up visits included in the fitting period?
- What happens if the first lens does not fit well?
- What are the costs for replacement lenses?
The best lens choice is not only a medical decision. It is also a practical decision about vision, comfort, cost, maintenance, and follow-up.
Common Myths About Astigmatism Corrective Lenses
“Astigmatism is a disease.”
False. Regular astigmatism is a prescription issue, not a medical condition. It is a measurable number that can often be corrected with the right lens while the lens is worn.
“Contacts cannot correct astigmatism.”
False. Toric contact lenses are designed specifically for this purpose, and many patients do well with them. If one toric lens rotates or blurs, that does not mean all toric lenses will fail; it may mean the fit, material, or brand needs adjusting.
“Screens cause regular astigmatism.”
False. Screen use can make dryness and fluctuating contact lens vision more noticeable, but it does not create regular astigmatism.
“Sitting close to a screen or book makes astigmatism worse.”
False. Sitting close may be a sign that the person is not seeing clearly, but it is not the cause of the prescription.
“Correcting the full prescription makes the eyes weaker.”
False. Full astigmatism correction can feel strong at first, and in some cases a doctor may introduce it gradually. That is an adaptation issue, not proof that the correction is damaging the eye.
“Glasses and contacts should feel exactly the same.”
False. Glasses sit in a frame in front of the eye. Contacts sit directly on the eye and move with it. The optics and comfort can differ, and the contact lens prescription may need to be adjusted separately from the glasses prescription.
“Corrective lenses cure astigmatism.”
False. Corrective lenses compensate for the way the eye focuses light while the lenses are being worn. They do not permanently change the shape of the eye.
“A very high prescription means I am legally blind.”
False. Legal blindness in the United States is defined as vision that cannot be corrected better than 20/200 in the better-seeing eye, even with glasses or contacts. A strong prescription that corrects well does not meet that definition.
“Eye rubbing can worsen astigmatism.”
True, but with an important distinction. Chronic, forceful eye rubbing can matter in some corneal conditions and is worth avoiding, especially if irregular astigmatism or keratoconus is a concern.
When to Return for a Fitting or Eye Exam
Astigmatism correction often needs refinement. Patients should return for evaluation if they have:
- persistent blur
- repeated toric lens movement or rotation
- glasses distortion that does not settle
- headaches or eye strain
- worsening dryness
- vision that does not match expectations after a reasonable trial
- contacts that repeatedly blur after blinking
- contacts that become noticeably worse later in the day
During the visit, the ophthalmologist or optometrist may check the prescription, cylinder, axis, frame fit, contact lens movement, lens rotation, deposits, lens material, tear film, and ocular surface health. Depending on the symptoms, testing may also include keratometry or corneal topography to measure the shape of the cornea more precisely.
For patients who have not had a recent comprehensive exam, a broader evaluation can also be useful because not every visual symptom is caused by astigmatism alone. Manhattan Eye’s guide to comprehensive eye exams in New York explains why the full eye health exam matters, not just the prescription check.
Contact Lens Symptoms That Need Prompt Care
Some contact lens symptoms should not be watched at home. Remove the contact lenses and contact an eye care professional promptly for:
- significant eye pain
- significant redness
- light sensitivity
- discharge
- sudden vision change
- severe discomfort
- blur that does not improve after removing the lens
Corneal ulcers are one reason contact lens symptoms should not be ignored. Patients should not try to decide on their own whether an irritated eye is serious based on appearance alone. If the eye is painful, red, light-sensitive, or vision is changing, it should be examined.
Quick Decision Guide: Glasses vs. Toric Contacts vs. Specialty Lenses
This table is a quick reference, not a substitute for a fitting or eye exam. The right choice depends on prescription, eye surface health, lens fit, lifestyle, budget, and safety.
| Option | Best fit | Visual stability | Dry eye considerations | Maintenance | Cost and coverage considerations | Fitting complexity |
| Glasses | Patients who want stable, low-maintenance correction | Very stable because the lens does not rotate on the eye | Often easier for dry eye than contacts | Low | Usually routine vision expense | Low |
| Soft toric contacts | Mild to moderate regular astigmatism with a healthy tear film | Good when the lens aligns well | Can fluctuate if dryness affects lens movement | Daily cleaning unless disposable | Often routine vision or out-of-pocket | Moderate |
| Daily disposable torics | Patients who want soft torics with fewer cleaning and deposit issues | Good when prescription and fit are available | Often helpful when deposits or hygiene are a concern | Lowest contact-lens maintenance | May cost more than reusable soft lenses | Moderate |
| Custom soft torics | Prescriptions outside common disposable ranges | Can be good when standard lenses are unavailable | Depends on material, fit, and tear film | Requires cleaning and replacement schedule | Higher cost than many standard soft lenses | Moderate to high |
| RGP lenses | Patients who need crisp optics or do poorly in soft torics | Often very sharp when tolerated | Can be less forgiving during adaptation | Custom reusable lens care | Higher upfront cost; coverage varies | High |
| Hybrid lenses | Patients who need rigid optics with a softer lens feel | Can be strong when fit is good | Depends on lens design and ocular surface | Custom reusable lens care | Higher upfront cost; coverage varies | High |
| Scleral lenses | Irregular astigmatism, dry eye, unstable vision, or selected regular astigmatism cases | Often very stable once fit is optimized | Can be helpful for selected dry eye patients | Custom reusable lens care | Often higher upfront cost; medical coverage may apply in selected cases | High |
If Glasses and Contacts Are No Longer Meeting Your Needs
Some patients do everything reasonably: they update their glasses, try toric contacts, change brands, treat dryness, and still feel limited by their vision or contact lens comfort. In that situation, the next step is to reassess the problem.
That may mean rechecking the prescription, reviewing the axis, evaluating the tear film, examining the cornea, reconsidering the contact lens fit, or discussing specialty lenses.
For selected patients, refractive surgery is worth discussing. Chronic contact lens intolerance, repeated infections, ongoing frustration, or a strong desire to reduce dependence on glasses and contacts are all reasonable reasons to explore surgical options. Candidacy depends on the prescription, corneal health, dry eye, and individual expectations.
Patients considering laser surgery or another refractive procedure should be evaluated for candidacy, corneal health, dry eye, prescription stability, and expectations. Depending on the eye, that discussion may include LASIK, SMILE, PRK, or an implantable lens option. Manhattan Eye has related guides on bladeless LASIK, SMILE eye surgery, and implantable collamer lenses for patients who want to understand those options in more detail.
The practical takeaway is this: astigmatism correction is not one-size-fits-all. If one lens option is not giving clear, comfortable, stable vision, that does not mean the astigmatism cannot be corrected. It means the correction may need to be refined, the eye surface may need attention, or a different lens category may fit the eye better.