SMILE Eye Surgery Basics: What It Is, How It Works, and What to Know First

Most people who start looking into SMILE laser eye surgery are already tired of glasses or contacts, and at least a little wary of LASIK surgery. They have done some reading, possibly encountered something alarming online, and want a clearer and calmer explanation of what this procedure actually is before deciding whether to pursue it. If that sounds like you, this article is written for you.
SMILE corrects nearsightedness and astigmatism by reshaping the cornea without cutting a flap. This structural difference from LASIK is what sets SMILE apart, and it is also where most of the questions begin.
Table of Contents
What Is SMILE Eye Surgery
SMILE stands for Small Incision Lenticule Extraction. A femtosecond laser creates a precisely shaped disc of tissue, called a lenticule, inside the cornea. The surgeon removes it through a small incision, typically two to four millimeters wide. Removing the lenticule changes the corneal shape, which changes how light is focused on the retina, which improves distance vision.
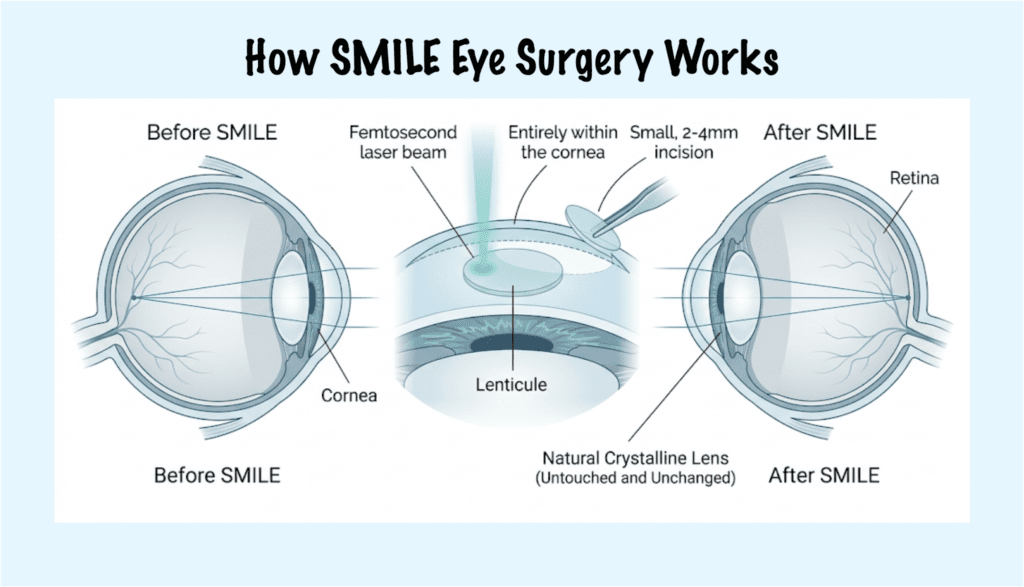
SMILE does not touch the natural lens inside the eye. The optics of the internal lens remain unchanged. Patients sometimes confuse this with procedures that implant or exchange a lens, but the SMILE procedure operates entirely on the cornea.
The procedure has been performed in Europe since the mid-2000s, with the early clinical development of refractive lenticule extraction and SMILE described in the peer-reviewed literature in 2008 and 2011. The original U.S. FDA approval for the ZEISS VisuMax Femtosecond Laser for SMILE was granted in September 2016. A faster version called SMILE Pro, using the VISUMAX 800 platform, received U.S. FDA approval in January 2024. “ReLEx SMILE,” which appears in some earlier research, is a previous name for the same approach.
How SMILE Works at a Basic Level
SMILE corrects nearsightedness, a refractive error in which the eye focuses light in front of the retina rather than directly on it. This happens when the eyeball is slightly too long or the cornea is too steep. The eyeball’s length cannot be changed, so the procedure works by reshaping the corneal surface to adjust how it bends light. Farsightedness, where light focuses behind the retina, is not addressed by SMILE in most current clinical applications.
In SMILE, a femtosecond laser creates a precisely shaped disc of tissue, the lenticule, inside the cornea. The shape and thickness of that disc are customized to each patient’s prescription. A cornea that needs more correction gets a lenticule with a different curvature than one that needs less. The amount of tissue removed determines how much the corneal shape changes, and that change determines the new focal power. The surgeon then removes the lenticule through a small incision, typically two to four millimeters wide.
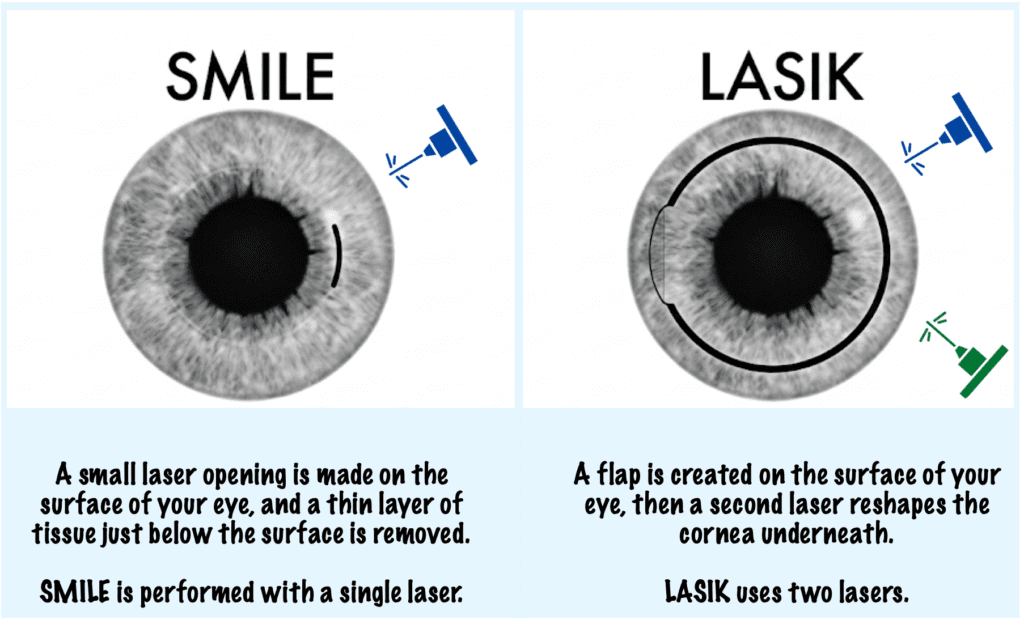
Unlike LASIK, which uses two lasers (one to create the flap and a second to ablate and reshape the cornea underneath), SMILE uses a single femtosecond laser to create the lenticule. The surgeon then extracts it manually through the small incision. There is no surface ablation and no second laser pass.
Because the reshaping happens entirely inside the corneal tissue, the outer corneal surface is never opened widely, which is what keeps the incision so small.
SMILE is not a surgery inside the eye. The procedure works on the cornea, which is the clear outer surface, and nothing behind it is involved. The natural lens, the retina, and the fluid pressure system of the eye are not touched. Patients sometimes worry that eye surgery raises the risk of glaucoma, macular degeneration, or cataracts. With SMILE, as with LASIK, those conditions are related to internal eye structures that the procedure does not reach.
What “Flapless” Really Means
To perform LASIK, a surgeon creates a large hinged flap that runs nearly all the way around the corneal surface, covering roughly 300 to 310 degrees of its circumference, almost a full circle. The flap is lifted, the cornea is reshaped underneath, and the flap is replaced. It heals through adherence and stays in the eye permanently.
In contrast, the access incision in SMILE is only two to four millimeters long, which works out to roughly 20 to 40 degrees of the corneal circumference. It is closer to a keyhole than a trapdoor.
That difference has clinical consequences. Because there is no flap, there are no flap-related complications. The nerve fibers in the outer corneal layers are disrupted far less than in LASIK, which is why the dry eye risk with SMILE is lower in most clinical comparisons. For patients with any degree of dry eye, who play contact sports, or who work in physically demanding environments, that is a practically meaningful distinction.
However, flapless does not mean incision-free and it does not mean risk-free. SMILE is real surgery, but the specific category of complications associated with a permanent corneal flap does not apply.
What Vision Problems SMILE Can Treat
SMILE primarily corrects myopia, or nearsightedness. It also addresses astigmatism in many patients, depending on the degree and the platform being used.
Astigmatism is a condition where the cornea is shaped more like an oval than a perfect sphere, which can cause blurred or distorted vision. Many patients with myopia and astigmatism within the treatable range are candidates for SMILE.
It is not used for farsightedness, also called hyperopia, in most current applications. In my practice, SMILE is often most straightforward once myopia gets above about -3.00 diopters, while very high myopia, often around -7.00 to -9.00 diopters and above, may prompt discussion of options like EVO ICL. Exact cutoffs still vary based on corneal anatomy, technology, and the full clinical picture, which is why the right choice should always be confirmed in a consultation.
Who Is a Good Candidate for SMILE Eye Surgery
While candidacy is determined by clinical measurement, the main requirements are prescription stability, healthy corneal anatomy, and overall eye health.
Prescription stability means no more than half a diopter of change over 12 months. Any laser vision correction procedure corrects a current prescription, not where the eyes may be heading. If the prescription is still moving, the timing is not right. A comprehensive eye exam or refractive consultation is the appropriate way to confirm stability history.
Corneal health is evaluated through topography, a detailed map of corneal shape and curvature, and by measuring corneal thickness. The cornea must be healthy enough in shape, symmetry, and thickness to safely yield the lenticule and maintain structural integrity afterward.
Eye health factors include the absence of active infections, corneal dystrophies, uncontrolled glaucoma, or conditions that would affect healing. Tear film is evaluated as well. Untreated dry eye affects measurement accuracy and recovery quality. Addressing it before surgery, rather than ruling out surgery, is usually the right approach. Options for managing dry eye range from lubricating drops to procedural interventions depending on severity.
A consultation with an eye surgeon who offers the full range of refractive procedures is the appropriate way to determine what candidacy actually looks like for your specific eyes.
Benefits and Tradeoffs of SMILE Eye Surgery
In SMILE, the flapless structure eliminates flap-related complications by design. For patients in contact sports, physically demanding work, or military service, the absence of a permanent corneal flap is a practical safety consideration.
The dry eye advantage is clinically real. SMILE disrupts fewer corneal nerve fibers than LASIK, so the reduction in tear film quality after surgery tends to be smaller. For patients with any existing dry eye, even mild or intermittent, SMILE is typically the more appropriate choice.
The smaller incision contributes to less post-procedure redness on the white of the eye and may support faster structural recovery.
Despite the benefits, SMILE is not for every patient. Like any refractive procedure, SMILE can involve both risks and temporary side effects, even though serious problems are uncommon. Outcomes depend on factors beyond the surgery itself: how the eye heals, whether any residual prescription remains, and how the brain adapts to new optics. The realistic expectation is vision as good as best-corrected vision in glasses or contacts, not necessarily better, and not identical for every person.
Procedural risks exist. If the lenticule is not created or removed exactly as planned, additional treatment may be needed. In rare cases, conversion to PRK may be required. These risks are manageable with an experienced surgeon, but they are real.
Key Benefits and Tradeoffs of SMILE Eye Surgery at a Glance
| Benefit | What to Know | |
| Flap | No flap, so no flap-related complications | Small incision still required |
| Dry eye | Lower risk than LASIK due to less nerve disruption | Still possible, particularly if pre-existing |
| Incision size | 2 to 4 mm vs. nearly full corneal circumference in LASIK | Not incision-free |
| Contact sports / physical activity | No permanent flap to displace | Standard post-op care still applies |
| Early visual recovery | Often recovers quickly. Many patients can function normally by the next day | Can be a bit cloudy or milky for the first 24 to 48 hours |
| Vision outcome | Typically matches best-corrected vision in glasses or contacts | Not guaranteed to be better; varies by individual |
| Procedural risk | Manageable with an experienced surgeon | Uncommon; when they occur, they are treatable with follow-up care |
| Enhancements | Touch-ups are uncommon | Usually handled with PRK or another planned approach, not by simply repeating SMILE in the same spot |
How SMILE Differs From LASIK and PRK
LASIK creates a large hinged flap across most of the corneal surface, reshapes the tissue underneath with an excimer laser, and replaces the flap. Two lasers are used. The flap stays in the eye permanently.
PRK removes the outer epithelial cell layer entirely, reshapes the corneal surface with an excimer laser, and allows the epithelium to regenerate over several days. There is no flap. Visual recovery is typically slower because the outer surface is regenerating. PRK is often appropriate for patients with thinner corneas or specific topography findings.
SMILE uses a single femtosecond laser to create a lenticule inside the cornea. The surgeon removes it through a two-to-four-millimeter incision. No flap, no surface ablation, one laser.
| Procedure | How the Cornea Is Accessed | Flap | Lasers Used |
| LASIK | Large-arc incision spanning ~300 degrees | Yes, permanent | Two (femtosecond + excimer) |
| PRK | Outer epithelial layer removed | No | One (excimer) |
| SMILE | Small incision, 2 to 4 mm | No | One (femtosecond) |
Patients with thin corneas may not be candidates for LASIK but may qualify for SMILE or PRK. For patients with very high prescriptions or corneas that are not suitable for any laser procedure, an implantable lens option is often the more appropriate path. Which procedure fits depends on anatomy and goals, and a consultation that covers the full range of options is the right place to work that out.
When to Take the Next Step
Once you have a basic understanding of what SMILE is and how it works, the natural next step is a refractive consultation. That is where general knowledge becomes specific to your eyes.
A consultation evaluates what no article can assess for you: corneal topography, prescription stability over time, tear film quality, corneal thickness, and overall anatomy. These measurements determine whether SMILE is appropriate for your specific eyes, and if not, which procedure would be a better fit.
When evaluating a surgeon, treat honest risk disclosure as a positive signal. A surgeon who names what can go wrong and explains how it is managed is demonstrating exactly the clinical judgment you want. One who tells you nothing can go wrong is not.
Going in with questions makes the consultation more useful. Some worth asking:
- Does the surgeon perform the full range of refractive procedures, including LASIK, SMILE, PRK, and implantable lens options? A surgeon who only offers one cannot give you a genuinely comparative recommendation.
- How many SMILE cases have they performed, and what does their complication experience look like?
- Given your prescription and anatomy, what would they personally recommend, and why?
One practical note if you wear contact lenses: most practices ask you to stop wearing them before measurements are taken. Soft lenses typically require three days out; lenses that correct astigmatism or rigid lenses require longer. Your practice will give you specific instructions, but factoring this into your scheduling avoids having to rebook.
It is also worth knowing that continuing in contact lenses long-term is not a consequence-free alternative. Contacts reduce the amount of oxygen reaching the corneal surface, increase the risk of infection, and are one of the more common contributors to the dry eye that many patients arrive with already. For many patients, the real comparison is not SMILE versus doing nothing. It is SMILE versus years of continued contact lens wear and its cumulative effects on the eye.
Questions That Come Up Before SMILE Eye Surgery
Some concerns are nearly universal among patients considering SMILE for the first time, and they are worth addressing directly.
The Permanence of SMILE Eye Surgery
Yes, the reshaping is permanent. The lenticule is removed and does not grow back. What concerns patients is usually not permanence itself but the irreversibility, the sense that there is no going back. Permanence is also what makes the result durable. An eye that was a good candidate for SMILE, with a stable prescription going in, does not tend to change back. What does change over time (near vision in your 40s, and eventually the internal lens) happens to every eye regardless of whether surgery was performed.
What If You Blink or Move During SMILE?
The fear of blinking or moving during the procedure is one patients often feel reluctant to voice. Modern laser systems track eye movement in real time and pause automatically if the eye moves outside a safe range. There is almost nothing the patient can do to interfere with the procedure. As I tell patients: just bring your eyeballs. The system handles the rest.
What the SMILE Docking Phase Feels Like
The answer depends on the platform being used. With the ZEISS VisuMax, which is what we use, there is no suction and no pressure. It is a touch technique: the laser system makes gentle contact with the eye surface, but nothing is pressed against the eye or held in place by suction. Patients using this system most often describe lights, some drops applied to the surface, and a brief awareness of contact. Some notice nothing at all. There is no pain. The anticipation is almost always worse than the procedure.
Is SMILE Eye Surgery Too New?
The question of whether SMILE is too new stems from comparing it to LASIK, which has been performed since the early 1990s. SMILE has been used in Europe since the mid-2000s and received U.S. FDA approval in 2016. The more useful measure is not years of existence but the volume of published clinical data and the experience of the surgeon performing it.
As a surgeon who trained with Professor Dan Reinstein, one of the pioneers of SMILE, I can say with confidence that this is not an experimental procedure. It has been in clinical use for years and is backed by a substantial track record.
Conclusion
If you are drawn to SMILE because it sounds minimally invasive compared to LASIK, that impression is based on a real structural difference. Its flapless design, small incision, and lower dry-eye burden are meaningful advantages for the right patient. Whether those differences make it the right choice for you depends on your eyes, not on the label alone.
FAQs About SMILE Eye Surgery
What does SMILE stand for?
Small Incision Lenticule Extraction.
Is SMILE too new to trust?
No, SMILE has been used in Europe since the mid-2000s and received U.S. FDA approval in 2016. SMILE Pro received U.S. FDA approval in January 2024. The published clinical literature is extensive.
Is SMILE permanent?
Yes. The corneal reshaping is permanent, and the lenticule does not grow back. However, natural vision changes can occur over time, including the gradual loss of near focus in your 40s or cataract development later in life that could require cataract surgery. These can happen regardless of whether a person has had refractive surgery. SMILE corrects the current distance prescription. It does not affect how the internal lens ages.
Will I need reading glasses after SMILE?
SMILE corrects current distance prescription. It does not prevent presbyopia, the gradual loss of near-focusing ability that develops in most people in their 40s. Reading glasses for close work in your 40s remain likely.
Can I have SMILE if I have astigmatism?
Many patients with myopia and astigmatism are candidates for SMILE. The degree of astigmatism that SMILE can address depends on the laser platform and your surgeon’s clinical assessment. A consultation will clarify whether your level falls within the treatable range.
What if I blink or move during the SMILE procedure?
Modern laser systems track eye movement in real time and pause if the eye moves beyond a safe threshold. The procedure does not depend on the patient holding perfectly still.
What does the pressure or suction feel like?
With the ZEISS VisuMax, there is no suction and no pressure. The system uses a touch technique: gentle contact with the eye surface, with nothing pressed against it or held by suction. Most patients describe lights, some eye drops applied to the surface, and a brief awareness of contact. Some notice nothing beyond that. There is no pain during SMILE.
What if SMILE is not right for me?
What is the difference between SMILE and SMILE Pro?
SMILE Pro uses an updated laser platform that creates the lenticule faster, shortening the docking phase of the procedure. The underlying approach is the same.
How should I think about negative SMILE stories online?
The brain treats vivid, specific accounts of harm as more urgent than statistics, even when the statistics give a more accurate picture. One detailed story will always feel more real than a summary of outcomes across thousands of patients. The visible sentiment in those communities is not a representative sample of outcomes.