Stye Removal and Treatment
A stye can feel minor at first, just a small, tender bump along the eyelid. But when the pain increases, the swelling lingers, or the lump keeps coming back, it quickly becomes more than a nuisance.
People are often told that styes are simple infections that resolve on their own. In reality, most styes are driven by blockage and inflammation of the eyelid’s oil glands, sometimes with secondary bacterial involvement that may require medical treatment.
This guide explains why some stys resolve quickly while others persist for months, and when home care is enough versus when medical treatment is appropriate. It also outlines what to expect from in-office procedures and how to reduce recurrence risk over time as part of long-term eye care.
Table of Contents
Why Styes Are Often Misunderstood
Many patients treat a stye as a minor infection that will resolve if they “leave it alone.” That assumption is one of the main reasons styes persist, recur, or become more frustrating than they need to be.
The “It’s Just a Small Infection” Myth
A stye is commonly framed as a simple bacterial infection. In reality, styes are often driven by gland blockage and inflammation, not infection alone. Styes may occur on the upper eyelid or lower lid depending on which gland is affected.
Because patients think of a stye as an infection, they expect a quick prescription drop, rapid disappearance, and no long-term management.
That is not how styes behave. Even when medication is started early, it reduces inflammation and bacterial load, but it does not immediately correct the underlying gland dysfunction.
Why Watchful Waiting Backfires
Watchful waiting can be reasonable for mild eyelid inflammation or blepharoconjunctivitis, but it is not ideal for a true stye. With a stye, early intervention tends to prevent:
- Gland scarring
- Transition into a chronic lump (chalazion)
- Months-long persistence
Large styes can persist for months if the underlying gland remains obstructed. In practice, some patients present six to nine months later with a persistent lump that never fully resolved.
The Cost of Doing “Half” the Treatment
Inconsistency prolongs the problem. Common patterns include:
- Skipping warm compresses
- Using medication intermittently
- Stopping hygiene once pain improves
- Using expired drops
- Applying treatment like a “quick fix” instead of a structured plan
Think of a stye as a fire: if you do not extinguish it properly at the start, it smolders. Incomplete early treatment often means longer steroid use, repeat courses, greater reliance on medication, and higher recurrence risk.
Why Bigger Styes Behave Differently
Small styes may resolve on their own, but larger ones behave differently. They:
- Carry more inflammatory load
- Tend to persist
- Often require procedural support (manual compression, debridement, or injection)
Medication in these cases reduces inflammatory load and may make procedural intervention easier. However, it does not simply dissolve the lesion overnight.
Who Should Be Treated Earlier
Certain patients warrant a lower threshold for active treatment:
- Immunocompromised individuals
- Patients with diabetes
- Children
- Those with recurrent styes
In these groups, delayed treatment increases the risk of progression to preseptal cellulitis or prolonged inflammation.
What Causes a Stye (and Why Some Keep Coming Back)
A stye does not occur at random. If you have had more than one stye, it usually reflects dysfunction of the oil-producing glands in the eyelid. A stye, medically called a hordeolum, develops when an eyelid oil gland becomes blocked and inflamed.
Some styes arise from infection of an eyelash follicle (external hordeolum), while others originate deeper within the meibomian glands (internal hordeolum). Bacteria may contribute, but obstruction and inflammation are typically the primary drivers.
A stye is different from:
- Chalazion: A firm, often painless lump that develops when a previously inflamed gland hardens and scars.
- A simple “pimple”: Eyelid glands are deeper, more structured, and behave differently than skin pores.
Pain, tenderness, and rapid onset favor a stye, which often presents as a painful bump along the lid margin. A slow-growing, painless lump is more likely a chalazion. The treatment options differs for each.
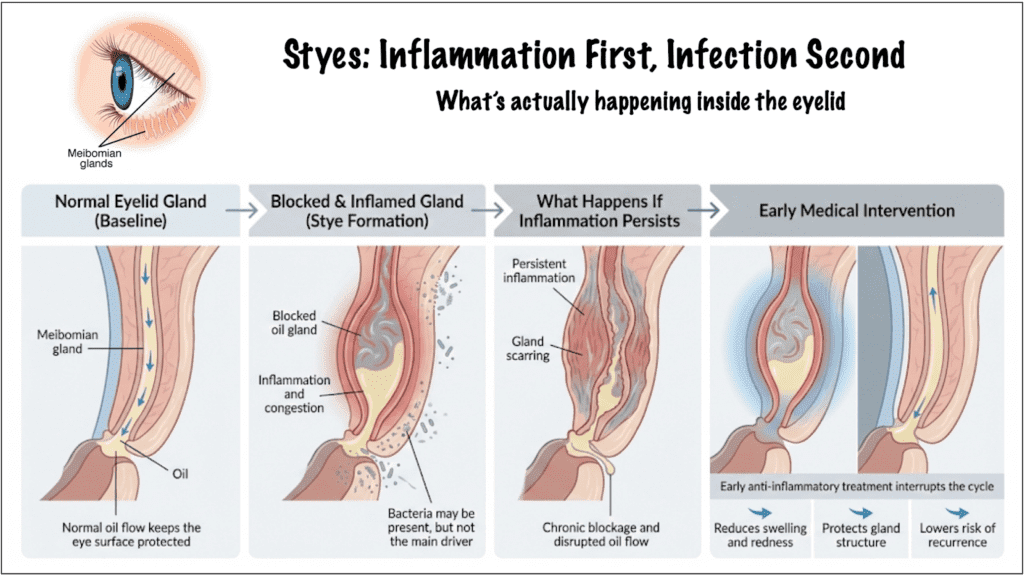
Infection vs. Inflammation
One of the most common misunderstandings is assuming a stye is purely infectious. It is not. In many cases:
- The gland is blocked.
- Oil cannot drain properly.
- Inflammation builds.
- Bacteria may secondarily worsen the process.
This is why antibiotic drops alone often do not “cure” the problem. If the gland remains obstructed, inflammation persists.
Why Some Keep Getting Them
Recurrent styes almost always signal underlying gland dysfunction. The most common contributors include:
- Blepharitis (chronic eyelid margin inflammation)
- Meibomian gland dysfunction (MGD)
- Rosacea
- Seborrheic dermatitis
- Acne-prone skin
- Poor eyelid hygiene habits
If you repeatedly develop styes in the same area, it usually indicates chronic blockage or structural changes that make that gland drain poorly. At that point, treating each stye as an isolated event is not enough. The focus has to shift toward restoring gland function and preventing the next episode.
The Role of Contact Lenses and Makeup
Contact lenses, eye makeup, and certain skincare products can increase risk by:
- Increasing bacterial load at the lid margin
- Physically clogging gland openings
- Contributing to inflammation
Improper replacement schedules or sleeping in lenses further increase risk. Makeup itself is not inherently dangerous, but old or contaminated products, especially mascara and eyeliner, can contribute to recurrence.
Systemic Risk Factors
Certain health conditions change how aggressively a stye should be treated. Patients with diabetes, immunocompromised states, or chronic inflammatory skin conditions can see faster progression rates with higher infection risk. In such cases, treatment thresholds are typically lower.
Why Some Styes Resolve Quickly, and Others Do Not
Small styes may decompress and drain naturally. Larger or recurrent ones may:
- Remain inflamed
- Harden into chalazia
- Scar the gland
- Persist for months
Once scarring occurs, recurrence risk increases because normal oil flow is disrupted.
This is one reason clinicians emphasize early, consistent treatment. The earlier the gland is decompressed and inflammation controlled, the less likely it is to harden into a long-lasting lump.
Are Styes Contagious?
Styes are not considered highly contagious in the way conjunctivitis can be. However, self-inoculation is possible. Rubbing the eye, poor hand hygiene, or contaminated cosmetics can spread bacteria to adjacent glands. Sharing medication is not recommended, even within households.
When Home Treatment Is Enough, and When It Is Not
If you have a stye, your first question is usually straightforward: Can this be managed at home, or is it time to see a doctor? The answer depends on size, pain, progression, and your risk profile.
For a small, early stye with mild tenderness and no spreading redness, initial home treatment is appropriate. The core components are as follows:
| Step | What to Do and Why | How to Do It Properly |
| Warm Compresses | Apply consistent heat to the eyelid. This softens thickened oil and promotes gland drainage | – Use a clean washcloth soaked in warm water (comfortably warm, not hot). – Keep in place for 8–10 minutes- Repeat 2–4 times daily – Avoid brief or lukewarm applications (ineffective) |
| Eyelid Hygiene (Foam or Lid Cleansers) | Clean the eyelid margin daily. This reduces bacterial load and debris that contribute to blockage and recurrence | – Use a designated lid cleanser or foam – Clean along the lash line gently but thoroughly – Perform consistently, even as symptoms improve |
| Avoid Irritation | Reduce additional stress on the gland. Prevents worsening inflammation and secondary infection | – Stop wearing contact lenses temporarily – Avoid eye makeup – Do not squeeze or puncture the stye – Never attempt to “pop” it, as this can increase inflammation and infection risk |
What Over-the-Counter Products Can and Cannot Do
Lubricating drops may improve comfort. However, antibiotic ointments without anti-inflammatory components are often limited in effect because inflammation, not infection alone, is driving the process. Heat and mechanical care remain the foundation.
When Home Treatment Is No Longer Enough
Seek medical evaluation if any of the following occur:
- The stye continues to enlarge after several days of proper home care
- Pain worsens instead of improving
- Redness spreads beyond the localized bump
- The eyelid becomes significantly swollen
- Vision becomes blurred or affected
- You have diabetes or are immunocompromised
Large styes often require more than compresses alone. Delaying treatment increases the likelihood of gland scarring or progression into a firm, persistent chalazion. Most styes are not emergencies, but worsening symptoms should not be ignored.
When Medication May Be Appropriate
Early use of topical antibiotic-steroid combination therapy can reduce inflammatory load and may prevent scarring when used appropriately. However, these medications are typically used for limited durations. They require monitoring due to potential pressure elevation from steroid components and are not instant cures. Consistency matters. Intermittent use prolongs recovery.
Oral Antibiotics: When They Are Used
Oral antibiotics are not routine for uncomplicated styes. They may be prescribed when:
- There is significant surrounding redness
- Preseptal cellulitis is suspected
- Infection extends beyond a localized gland
Doxycycline may also be used longer-term in recurrent cases for its anti-inflammatory effects, particularly in patients with gland dysfunction or rosacea.
A Practical Threshold
If there is no meaningful improvement within 3–5 days of proper compresses and lid hygiene, or if symptoms worsen at any point, it is reasonable to seek evaluation. Early intervention often shortens the overall course and reduces recurrence risk.
Professional Stye Treatment and Removal: What to Expect
When home care and prescription drops are not enough, treatment shifts from reducing inflammation to actively clearing the blocked gland.
How Doctors Decide to Escalate
Escalation is usually considered when:
- The lesion remains large or firm after appropriate medication
- The stye has hardened into a chalazion
- Symptoms persist despite consistent home care and prescribed treatment
- Recurrence is frequent
At this stage, the goal is to restore drainage and prevent structural damage to the gland.
Manual Gland Expression or Debridement
In many cases, the first step is mechanical. This directly addresses obstruction, which medication alone cannot always resolve. The process may involve clearing debris from the lid margin or manually expressing the blocked gland.
These are performed in-office and typically take only a few minutes. It may feel uncomfortable, but it is brief. Many patients notice gradual improvement over the following days.
Incision and Drainage
If the lesion is large, persistent, or firm, in-office procedure may be recommended. A stye surgery is a minor procedure that involves local anesthesia and a small incision on the inner eyelid surface to drain the trapped material.
The procedure is short. Mild swelling or bruising can occur for several days. Most patients resume normal activity quickly. This is not usually the first-line step for early styes. It is reserved for those that fail conservative therapy.
Steroid Injection
For certain firm chalazia, a steroid injection may reduce inflammation and shrink the lesion without surgical drainage. Results are gradual rather than immediate.
Recurrent Styes: Changing the Strategy
If styes continue to return, repeated eye drops are not the long-term solution. At that point, the focus shifts toward gland rehabilitation. This can include:
- Thermal gland therapies
- Intense pulsed light (IPL)
- Radiofrequency-based treatments
- Lid margin debridement
These in-office preventive therapies are typically considered in recurrent disease or documented gland dysfunction, not for a first uncomplicated stye. These aim to improve oil quality and restore gland architecture, not simply suppress each flare.
Setting Expectations
Even with professional treatment, large lesions may take weeks to fully flatten. A second round of therapy is sometimes necessary, and improvement is gradual. The objective is durable resolution, not overnight disappearance.
Risks, Complications, and What Happens If You Wait Too Long
Most styes are localized and self-limited. However, delaying appropriate treatment can change how they behave.
What Typically Happens If a Stye Is Left Alone
When a stye is left alone, one of three things occurs:
- It drains and resolves
- It partially improves but leaves a firm lump
- It hardens into a chalazion
When inflammation persists, the blocked gland can scar. Once scarring occurs, normal oil flow may not fully recover, increasing the likelihood of recurrence in that location. This is why early decompression and inflammation control matter.
When a Stye Becomes a Chalazion
A painful, tender bump may gradually become less painful, firmer, and more defined. At this stage, the sharp tenderness often fades, but the residual blockage and inflammation can remain. Chalazia are not dangerous, but they can persist for months without intervention.
Warning Signs of Something More Serious
Although uncommon, a stye can progress beyond a localized gland. Seek prompt evaluation if you develop any of the following:
- Rapidly spreading redness
- Increasing eyelid swelling
- Fever
- Significant tenderness around the entire eyelid
- Difficulty opening the eye
These signs may indicate preseptal cellulitis, an infection of the surrounding eyelid tissue that requires systemic treatment.
Can a Stye Affect Vision?
Direct vision loss from a stye is rare. However, vision may feel blurred temporarily if:
- The eyelid is significantly swollen
- The lesion presses on the cornea
- Ointments are being used
Persistent visual disturbance should always be evaluated.
When a Persistent Lump Needs Further Investigation
If a lump persists despite appropriate treatment, recurs repeatedly in the exact same location, or has an atypical appearance, further evaluation may be necessary to rule out less common eye conditions. In rare cases, a biopsy is considered. This is uncommon, but persistent, non-resolving lesions should not be ignored.
Who Is at Higher Risk for Complications
Complications are more likely in patients with diabetes, immunocompromised individuals, and children who rub or manipulate the lesion. In these groups, doctors often intervene earlier.
Putting Risk in Perspective
Serious complications are not the norm. Most styes resolve without long-term consequences when treated appropriately. The key risk is not a catastrophe. It is chronicity — scarring, recurrence, and prolonged inflammation. Early, consistent management reduces that risk substantially.
Preventing Recurrence and Knowing When to See an Ophthalmologist
Recurrence is rarely random. It usually reflects ongoing gland dysfunction that requires consistent maintenance. If you have had more than one stye, the goal shifts from treating the current bump to preventing the next one.
Why Some People Keep Getting Styes
Patients who experience repeated styes often have:
- Chronic blepharitis
- Meibomian gland dysfunction (MGD)
- Rosacea or acne-related inflammation
- Inconsistent eyelid hygiene
In these cases, the issue is not a single blocked gland. It is a pattern of poor oil drainage across multiple glands. Treating each flare without addressing gland health increases the likelihood of future episodes.
The Most Effective Daily Prevention
The foundation of prevention is mechanical, not pharmaceutical. This involves:
- Ongoing Warm Compresses: even after the stye resolves, periodic heat helps maintain oil flow and prevent thickening. For patients prone to recurrence, this is often recommended several times per week.
- Lid Margin Hygiene: Regular cleansing of the lash line reduces debris and bacterial load. This is particularly important in patients with blepharitis or MGD.
Adjusting Makeup and Contact Lens Habits
After a stye:
- Replace mascara and liquid eyeliner
- Avoid old or expired products
- Do not share cosmetics
- Follow proper contact lens replacement schedules
- Avoid sleeping in lenses unless specifically prescribed
Small hygiene adjustments can significantly reduce recurrence risk.
When Office-Based Preventive Therapies Are Considered
In patients with chronic recurrence, mechanical at-home care may not be sufficient. In such cases, preventive in-office treatment plans are considered, including:
- Thermal gland therapies
- Intense pulsed light (IPL)
- Radiofrequency treatments
- Lid margin debridement
These approaches aim to improve oil quality, clear gland obstruction, and restore normal gland architecture rather than repeatedly treating inflammation. They are typically considered when recurrence is frequent or persistent.
When to See an Ophthalmologist Instead of Primary Care
If the diagnosis is uncertain, an eye doctor can determine whether the lesion is a stye, chalazion, or another eyelid condition. Both optometrists and ophthalmologists evaluate styes, but referral to an ophthalmologist is appropriate when:
- Styes are recurrent despite proper home care
- A lump persists beyond several weeks
- The lesion has atypical features
- There is concern for structural gland damage
- Episodes are frequent and affecting quality of life
Specialist evaluation is also appropriate for patients with diabetes, immunocompromised states, or underlying inflammatory skin disease.
A Practical Prevention Principle
If you could focus on one thing to reduce future styes, it would be this: Maintain gland function before inflammation begins. That means consistent heat, lid hygiene, and early evaluation when symptoms start — not waiting for a large, painful lesion to develop.
Most recurrent styes are preventable with structured maintenance and timely intervention.