Implantable Collamer Lens (ICL) Surgery: A Decision Guide
If you are considering Implantable Collamer Lens (ICL) surgery, you are likely already deep into research about your vision problems and correction options. You may have been told you are not an ideal LASIK candidate. You may have high myopia and thick glasses. Or you may simply want the sharpest vision possible without compromising your cornea.
ICL is not a “better LASIK.” It is a different category of surgery.
Instead of reshaping the cornea with a laser, ICL involves placing a custom-designed, biocompatible lens inside the eye, behind the iris and in front of your natural lens. The cornea is left untouched. The optics are powerful. The outcomes can be remarkable.
But this is intraocular surgery.
That means there are real trade-offs, and your baseline eye health matters. There are different risks, different visual side effects, and a different long-term profile compared to laser vision correction.
In my practice, I perform LASIK, SMILE, PRK, ICL, and refractive lens exchange. As an eye doctor, when I recommend a procedure, it is not because it is the only one I offer but because, for that specific patient, it is the best option.
This guide condenses how I counsel patients in my office, what I explain before surgery, what I watch for after surgery, and what I wish more people understood before making this decision.
ICL can be life-changing. It can also require patience, careful selection, and realistic expectations.
Let’s walk through it properly.
Table of Contents
Who ICL Is For (and Who It Is Not)
While ICL is an excellent option, it is not for everyone. A good candidate is someone whose anatomy, measurements, and expectations align with an intraocular solution. In my practice, the strongest ICL candidates tend to fall into one of a few categories.
1. Patients with Moderate to High Myopia
ICL performs particularly well in higher prescriptions. The more cornea that needs to be removed for laser surgery, the more I begin to favor an intraocular solution.
For patients in the -6, -8, -10 range and beyond, preserving the cornea becomes increasingly important. With higher laser corrections, you remove more tissue. That can affect optical quality and long-term structural integrity. With ICL, the cornea is left untouched.
For these patients, the visual clarity can be excellent, and the satisfaction rates are very high.
2. Patients Who Are Not Ideal Laser Candidates
There are patients with thin corneas, irregular corneas, or prescriptions that sit at the edge of what laser surgery can safely treat. For them, ICL is not a second-best option. It is often the better option. If someone is not a safe candidate for LASIK or SMILE, the decision becomes straightforward. I move toward ICL.
3. Patients Concerned About Dry Eye
Laser procedures reshape the cornea and can disrupt corneal nerves. Dry eye can occur, particularly with LASIK.
ICL does not alter the corneal surface. In my experience, patients undergoing ICL have significantly less dry eye burden compared to laser-based procedures.
If someone already has marginal tear film stability or a history of dry eye symptoms, that may influence the decision.
4. Patients Who Value Corneal Preservation Long-Term
One under-discussed benefit of ICL is future flexibility. When patients eventually reach cataract age, having an untouched cornea can simplify lens calculations and expand options. While cataract surgery is decades away for most ICL candidates, preserving corneal integrity today can matter later.
Who Is Not a Good ICL Candidate?
ICL is intraocular surgery. That alone excludes certain patients. I am cautious in patients who:
- Have unstable refractions
- Cannot discontinue contact lenses long enough for accurate measurements
- Have poorly controlled ocular surface disease
- Have unrealistic expectations about perfection or reversibility
- Are unwilling to attend structured post-operative follow-ups
Additionally, while serious complications are rare, ICL carries intraocular risks. There is a small but real risk of inflammation, pressure elevation, endothelial damage, and lens-related cataract formation.
This is not the same risk profile as laser surgery. It is a different one. Patients must be comfortable accepting that category of risk.
The right ICL candidate understands that this is a surgical implant inside the eye, not a cosmetic tweak. They want strong optical quality, are comfortable with intraocular surgery, and value preserving their cornea.
When those factors align, ICL can be one of the most rewarding procedures we perform.
ICL vs LASIK/PRK/SMILE: The Trade-Off Matrix
When a patient is eligible for both ICL and laser vision correction procedures, the decision ultimately comes down to where the risk lives and which trade-offs the patient is comfortable accepting.
Because I perform LASIK, SMILE, PRK, ICL, and refractive lens exchange, my recommendation is not tied to a single procedure. It is based on what truly fits that individual patient’s anatomy, lifestyle, and priorities.
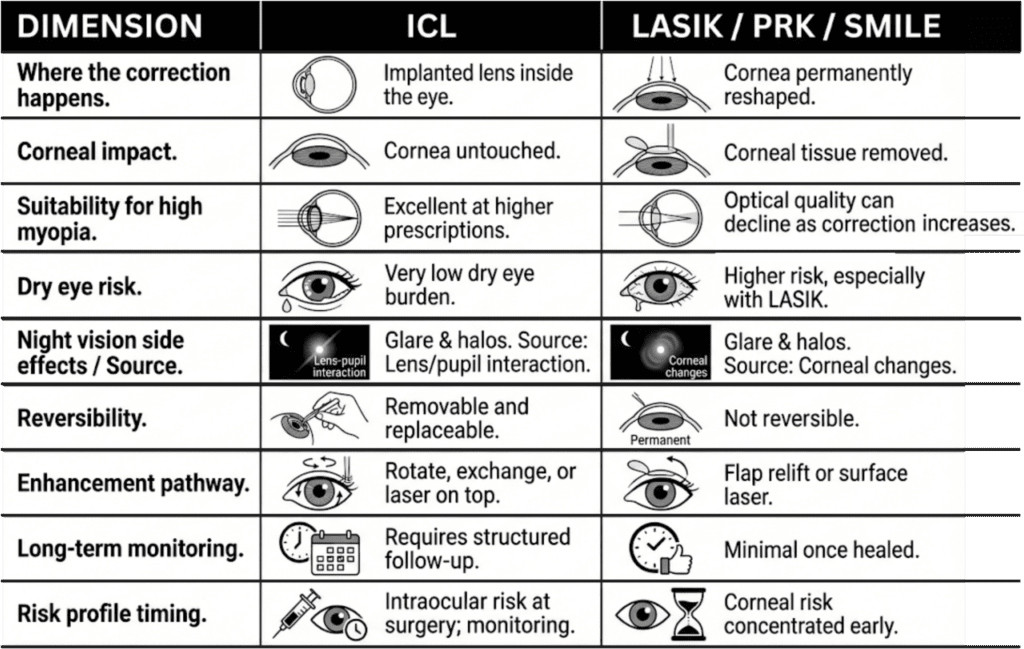
This is how I explain the differences:
| Dimension | ICL | LASIK / PRK / SMILE |
| Where the correction happens | Implantable lens placed inside the eye | Cornea permanently reshaped |
| Corneal impact | Cornea untouched | Corneal tissue removed (ablated or carved) |
| Suitability for high myopia | Performs exceptionally well at higher prescriptions | Optical quality can decline as the correction increases |
| Dry eye risk | Very low dry eye burden compared to corneal laser procedures in my experience | Higher risk, especially with LASIK |
| Night vision side effects | Can include glare and halos | Can include glare and halos |
| Source of visual artifacts | Lens–pupil interaction | Corneal surface changes / higher-order aberrations |
| Reversibility | Removable and replaceable | Not reversible |
| Enhancement pathway | Rotate, exchange, or laser on top | Flap relift or surface laser |
| Long-term monitoring | Requires structured follow-up appointments (pressure, vault, healing, symptoms). | Minimal once healed |
| Risk profile timing | Intraocular risk at time of surgery; monitoring over time | Corneal risk concentrated early |
The Core Trade-Off
Laser surgery reshapes the cornea. ICL leaves the cornea alone and places a custom lens inside the eye.
Because ICL is an intraocular surgery, it carries a different category of risk. There is a small but real possibility of inflammation, pressure elevation, endothelial cell loss, or cataract formation. Although rare, these are intraocular risks, not corneal ones.
While laser surgery does not carry those intraocular risks, it permanently alters corneal tissue and can induce dry eye or higher-order aberrations, particularly in higher prescriptions.
If someone is -8, -10, or higher, I begin to favor ICL because preserving corneal integrity becomes increasingly important.
Dry Eye Considerations
In my experience, dry eye risk follows a clear hierarchy:
LASIK > PRK > SMILE > ICL
ICL does not disrupt corneal nerves. Patients undergoing ICL generally have far less dry eye burden compared to corneal laser procedures. This matters to patients who already struggle with marginal tear film stability.
Visual Artifacts
Both laser procedures and ICL can produce glare and halos. With laser surgery, these are often related to corneal surface changes or higher-order aberrations.
With ICL, glare appears to be related to lens–pupil interaction. I have seen a significant amount of nighttime glare in some ICL patients, sometimes requiring pupil-constricting drops such as brimonidine. In many cases, this improves with time, but occasionally it persists.
Because the mechanism is different, the experience can be different. Some patients adapt quickly. Others are more sensitive. Tolerance and expectations matter.
Residual Prescription and Enhancements
In my practice, I expect similar refractive accuracy from ICL and laser procedures when measurements are done properly. In ophthalmology, outcomes hinge on measurement discipline as much as technology.
If there is residual astigmatism with ICL, particularly in toric lenses, rotation is often the first step. With laser procedures, enhancement typically involves relifting the flap or performing surface ablation.
My threshold for enhancement is high with both. Going back into an eye, whether intraocularly or lifting a flap, is not something I take lightly.
That said, true residual errors are uncommon when pre-operative measurements are stable and the ocular surface is optimized. Most patients achieve the clarity we aim for without needing additional procedures. When enhancement is necessary, it is approached deliberately and only when the potential visual gain clearly outweighs the additional surgical risk.
Reversibility
ICL is removable and replaceable. Laser surgery is not. However, this does not mean removal is trivial or something to rely on casually. It means that if necessary, the lens can be exchanged or removed in a controlled surgical setting. For some patients, that optionality is reassuring.
Cost and Logistics
ICL is typically more expensive. The lens itself has a cost, and the procedure often involves a surgery center and anesthesia. Laser procedures are generally simpler from a logistics standpoint. Many patients have same-day surgery and go home shortly afterward. For some patients, this becomes part of the decision.
How I Frame the Decision
If someone is a moderate myope with a healthy cornea and no dry eye, both options may be reasonable.
If someone has high myopia, marginal corneal thickness, or strong dry eye concerns, ICL often becomes the stronger choice.
The decision is personal. It depends on risk tolerance, anatomy, lifestyle, and long-term priorities. ICL is not a better LASIK. It is a different category of surgery with a different risk profile and different benefits.
Lens Design Choices That Matter More Than Patients Are Told
Patients often assume that choosing an ICL is similar to choosing a brand or model. In reality, modern ICL selection is far more standardized and anatomy-driven than most people realize.
The ICL is a type of phakic intraocular lens made from Collamer, a collagen-based copolymer designed for long-term biocompatibility inside the eye. It sits behind the iris and in front of your eye’s natural lens. Its optical effect is purely refractive, bending light so it focuses properly on the retina without removing corneal tissue.
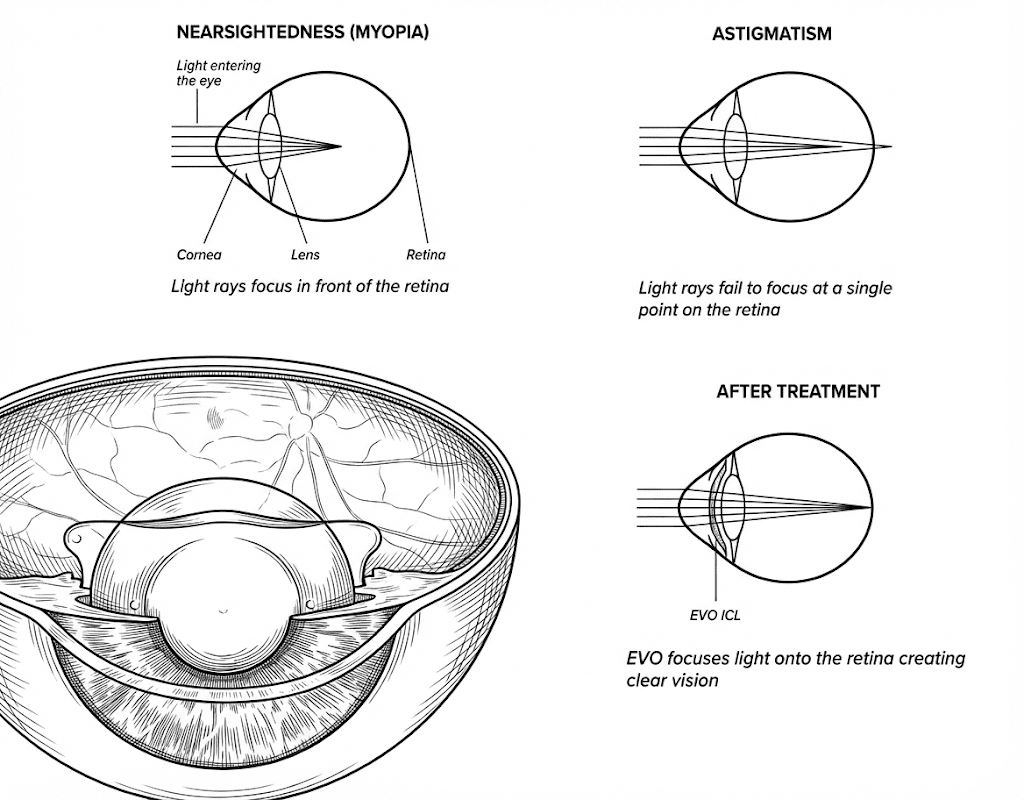
The current-generation EVO ICL is the standard platform (FDA-approved in the United States). Older versions that required an iridotomy are no longer routinely used. The central port design allows natural fluid flow and eliminates the need to create a hole in the iris. There is not a menu of dramatically different lens “types” for patients to shop between. What matters is not brand selection but precision.
Sizing and Vault: The Invisible Variable
Sizing is one of the most critical variables in ICL surgery. The lens must sit behind the iris and in front of the eye’s natural lens at an appropriate distance. This spacing is called the vault. Modern nomograms and biometric measurements make vault prediction highly reliable.
In my experience, vault is very predictable when measurements are done properly. However, even with excellent planning, biological variability exists. A lens that measures perfectly preoperatively can sit slightly differently once inside the eye.
- When vault is too low, there is concern about contact with the natural lens.
- When vault is too high, rotation or pressure changes can occur.
These are rare, but they are part of the design considerations.
Toric vs. Non-Toric: Astigmatism Complexity
In patients with significant astigmatism, a toric ICL is used. The lens must be aligned precisely along the correct axis. Even small degrees of rotation reduce astigmatic correction.
Axis marking today is very accurate. The larger variable is whether the lens rotates after implantation. If rotation occurs, it can usually be corrected surgically. This is one of the few lens-related variables that patients may notice postoperatively if residual astigmatism remains.
Pupil Size and Optical Zone
Pupil size matters in every refractive procedure, not just ICL. In low-light conditions, large pupils can interact differently with the optical zone of the lens. In some patients, this contributes to nighttime glare.
We measure scotopic pupil size preoperatively, but it does not always perfectly predict who will experience glare. Some patients with large pupils have no symptoms. Others with average pupils notice more disturbance.
This is one of the areas where individual neuroadaptation plays a role.
What Patients Often Misunderstand
Patients sometimes think lens selection is purely technical — a number entered into a machine. In reality, there is an element of clinical judgment:
- Age matters.
- Lifestyle matters.
- Whether someone spends all day on a computer matters.
- Whether someone is extremely sensitive to visual imperfections matters.
This is similar to refractive laser planning. It is not just about hitting 20/20. It is about aligning the optical outcome with how the patient actually lives.
The Bottom Line
Modern ICL surgery is highly customized, but not in a consumer-facing way. The customization happens in measurement, nomograms, vault prediction, and surgical planning. It does not happen through brand selection.
What ultimately matters more than the “type” of lens is:
- Accurate preoperative refraction
- Stable ocular surface
- Correct sizing
- Proper alignment
- Careful follow-up
When those are done well, the lens itself is remarkably reliable.
ICL Surgery: What Is Predictable and What Is Not
Modern ICL surgery is remarkably precise. When measurements are done correctly and the ocular surface is optimized, most outcomes are highly predictable. Still, there are variables we cannot fully control.
What Is Predictable
- Vault is highly predictable with modern nomograms and biometric measurements. In most cases, the lens sits exactly where we expect it to.
- Immediate refractive correction is also very predictable. Once the dilation wears off, many patients are already seeing extremely well, sometimes 20/20 or better.
- When pre-operative refractions are stable and contact lenses have been discontinued appropriately, refractive accuracy is excellent.
From a surgical standpoint, this is not guesswork. It is planned, measured, and executed with precision.
What Remains Variable
Even technically perfect eye surgery does not guarantee perfect subjective vision. I have seen cases where the lens is perfectly centered, vault is ideal, and the patient reads 20/15 in the office — yet something feels “slightly off” to them in daily life.
There are a few reasons for this:
- Subtle residual astigmatism can be more noticeable in ICL than in laser procedures
- Pupil dynamics differ in real-world lighting
- Neural adaptation varies from patient to patient
In other words, objective metrics do not always match subjective experience. The difference between anatomical success and perceived visual quality can be difficult to explain, but it is real.
The Limits of Control
Patients sometimes assume that surgical precision equals total control over the outcome. As a surgeon, I control measurements, lens power selection and the surgical technique. What I cannot fully control is biological variability, how the lens settles, and how the brain adapts to new optics. While this is true for all refractive procedures, patients sometimes underestimate it with ICL because the optics are so strong and the early visual results can be dramatic.
A Balanced Reality
When done properly, ICL surgery is one of the most accurate refractive procedures we perform. But surgery is not the final step in vision. Achieving a better vision is both an optical and a neurological process. Healing, adaptation, and perception continue afterward. That does not mean something is wrong. Understanding this distinction before surgery prevents unnecessary anxiety later.
Early Recovery Is Not the Same as Visual Stabilization
One of the most common misunderstandings about ICL surgery is the belief that early clarity equals final outcome. They are not the same thing, and full recovery time can vary.
The First Few Days: What Is Normal
In the first days after surgery, several temporary changes can occur:
- Pupils may not constrict evenly right away
- Mild inflammation can be present
- Vision can fluctuate slightly
- Pressure is monitored closely (particularly in patients with risk factors for glaucoma or pressure sensitivity)
We use eye drops (often including steroids) to control inflammation. Pressure is checked early and repeatedly. If something is truly wrong, it is typically detected in this early window.
Most patients see very well almost immediately. While that part is reassuring, clarity during an eye exam does not mean the visual system has fully stabilized.
Early Follow-Ups: What “Everything Looks Fine” Actually Means
At one week or one month, patients are often told that everything looks perfect. From a structural standpoint, that is usually true.
- The lens is centered.
- The vault is appropriate.
- The cornea is clear.
- The pressure is normal.
What that does not mean is that the brain has fully adapted to the new optics or that subtle visual disturbances have settled. Structural stability and perceptual comfort do not always evolve at the same speed.
The Neuroadaptation Timeline
Neuroadaptation is highly individual. Some patients adapt almost immediately. Others take weeks. Some take months, and occasionally, it can take up to a year.
There is currently no reliable way to predict who will adapt quickly and who will need more time.
This variability is one of the most difficult aspects to counsel, because early vision can be objectively excellent while the patient still feels something is “different.”
Surface Stability Matters More Than Patients Realize
A healthy ocular surface is essential during this phase. Even subtle tear film instability can amplify glare, ghosting, or fluctuation.
Many patients insist they do not have dry eye because they do not feel burning or irritation. That does not mean the surface is stable. Optimizing the tear film can significantly improve the quality of vision during this adaptation window.
When to Be Concerned
Fluctuation alone in the first few weeks is not alarming. What warrants closer evaluation:
- Persistent or worsening glare that impacts function
- Increasing pressure
- Progressive residual refractive error
- Signs of inflammation
These are uncommon, but they are monitored deliberately.
The Reality
Early recovery is about healing, while visual stabilization is about integration. They overlap, but they are not identical processes. Understanding this before surgery prevents premature regret during the first few months.
Visual Side Effects, Explained Without Euphemisms
Every refractive procedure involves optical trade-offs. ICL is no exception. Most patients have minimal or no significant visual disturbances. But when side effects occur, they are real and should be discussed plainly.
Halos, Glare, Rings, and Ghosting: What Are We Talking About?
Patients often use these terms interchangeably, but they are not identical.
- Halos: Circular light around bright sources
- Glare: Light scatter that reduces contrast
- Starbursts: Radiating streaks from lights
- Ghosting: A faint duplicate or shadow image
In ICL surgery, the most common long-term complaint is nighttime glare. This can present as halos around headlights, increased sensitivity to bright light in low-light settings, or difficulty with night driving.
Why Does It Happen?
With laser surgery, glare and halos are often related to corneal surface irregularities or higher-order aberrations. With ICL, the mechanism appears different. It is likely related to lens–pupil interaction in dim lighting.
Patients with large pupils tend to report more symptoms, although pupil size alone does not perfectly predict who will struggle. In some cases, we use pupil-constricting drops such as brimonidine to reduce nighttime glare. This can help, but it is not a universal solution.
How Common and How Long?
In my experience, the majority of patients do not experience significant long-term visual disturbances. For those who do, the intensity often decreases over time as the brain adapts. Improvement can occur over weeks or months. Occasionally, it can take up to a year. There are cases where some degree of glare persists. That is uncommon, but it is possible.
Daytime vs Nighttime Vision
Many patients who report glare still see extremely well in normal daylight conditions. The challenge typically appears in:
- Night driving
- Low-contrast environments
- Dark rooms with isolated bright light sources
A patient can measure 20/20 or better in the clinic and still feel uncomfortable at night. That does not mean the surgery failed. It means the optical experience is different.
When Side Effects Require Action
Visual disturbances become clinically significant when they:
- Persist beyond the expected adaptation window
- Interfere with driving or occupational demands
- Cause meaningful anxiety or avoidance behavior
In those cases, we reassess.
- We evaluate residual refractive error.
- We evaluate the ocular surface.
- We assess pupil dynamics.
- We determine whether conservative management, medication, or surgical adjustment is appropriate.
The Honest Perspective
ICL can deliver exceptional clarity, especially in higher prescriptions. But clarity and visual comfort are not always identical. For most patients, side effects are mild or diminish with time. For a small subset, they require active management.
Neuroadaptation: What It Is, What It Isn’t, and Who Struggles
Neuroadaptation is one of the most misunderstood aspects of ICL surgery. It is not a defect in the lens. It is not something “going wrong.” It is the brain adjusting to a new optical system.
What Neuroadaptation Means
After ICL implantation, light is entering the eye through a different optical pathway than it did before. Even when the refractive correction is precise, the brain still needs time to recalibrate how it interprets that signal.
For some patients, this adjustment is nearly immediate. For others, it takes time.
This is especially relevant when it comes to glare, halos, or subtle contrast changes. The optical input may be technically clear, but it feels unfamiliar. With time, the brain often filters or deprioritizes those signals.
What Neuroadaptation Does Not Mean
Neuroadaptation is not a cure-all explanation. If there is significant residual refractive error, unstable pressure, inflammation, or vault problems, those need to be addressed directly.
It is also not a guarantee that every visual disturbance will disappear. Some symptoms improve substantially. Some partially improve. A small minority may persist.
Who Struggles More?
There is no reliable pre-operative test that predicts who will struggle with adaptation. Patients with larger pupils may report more glare, but pupil size alone does not determine outcome. In my experience, the following can influence adaptation:
- Ocular surface instability
- Residual astigmatism
- Heightened sensitivity to visual imperfections
- High visual demands, particularly night driving
But none of these are absolute predictors. Some patients with ideal measurements struggle, while others with apparent risk factors adapt quickly.
Timeline Expectations
Neuroadaptation can occur within weeks. It often continues over several months. In some cases, improvement can still be seen at the one-year mark. That variability can be frustrating and requires patience.
The Practical Approach
When patients report visual disturbances early on, we do not immediately assume failure. We first:
- Optimize the ocular surface
- Confirm refractive stability
- Recheck vault and lens position
- Monitor pressure
If all structural parameters are sound, time is often part of the solution. Most patients adapt. A small percentage require additional intervention.
Residual Prescription: How Common, How Much Is Acceptable
One of the most common fears patients have is waking up after surgery and still needing glasses. That concern is reasonable. With proper pre-operative measurements and a stable ocular surface, significant residual refractive error after ICL is uncommon.
How Common Is Residual Error?
In my practice, when patients have discontinued contact lenses appropriately and the refraction is stable, outcomes are highly accurate.
ICL is not inherently less precise than laser surgery; refractive accuracy largely reflects the quality of the pre-operative refraction. If the measurements are precise, the outcome is usually precise.
Residual astigmatism or small refractive shifts can occur, but large unexpected misses are not typical.
What Is Considered “Acceptable”?
Acceptability is patient-dependent. Clinically, very small residual refractive errors, such as 0.25 or 0.50 diopters, may not meaningfully change vision.
But perception varies.
Some patients tolerate small residual astigmatism easily. Others are highly sensitive to even minor imperfections. Subtle astigmatism can feel more noticeable to some patients after ICL than after laser correction.
That is not because the surgery failed. It reflects how different optical systems are perceived.
When Does It Require Action?
I do not recommend enhancement casually. If a patient has measurable residual refractive error, we first determine:
- Is the refraction stable?
- Does correcting it in trial lenses meaningfully improve vision?
- Is the patient functionally limited?
If trial correction does not significantly improve clarity, surgery is unlikely to provide meaningful benefit.
When enhancement is necessary, options may include:
- Rotating a toric lens
- Exchanging the lens
- Performing laser correction on top
Each carries additional risk. That risk must be justified by real visual gain.
Who Is at Higher Risk for Residual Error?
Certain factors increase variability:
- Long-term rigid contact lens wear
- Unstable tear film
- Inconsistent pre-operative refractions
- Fluctuating measurements
This is why contact lens discontinuation and ocular surface optimization are not optional. They directly affect surgical accuracy.
The Bottom Line
Residual prescription after ICL is not expected when measurements are stable and planning is meticulous. Small residual amounts can occur. Whether they matter depends less on the number and more on the patient’s visual demands and sensitivity. Precision matters. Perception matters just as much.
Enhancement Paths: PRK, LASIK, Lens Rotation, Exchange
When a patient is unhappy after ICL surgery, the instinct may be to “fix it quickly.” That is not how I approach it. Enhancement is never automatic. It is deliberate.
First Step: Confirm the Diagnosis
Before discussing any additional surgery, we determine:
- Is the refraction stable?
- Does trial lens correction meaningfully improve clarity?
- Is the ocular surface optimized?
- Is the vault appropriate?
- Is the lens properly aligned?
Many early complaints improve with time, surface optimization, or neuroadaptation. Not every symptom requires another procedure.
Lens Rotation: The First-Line Fix for Toric ICL
In toric ICL cases, residual astigmatism is most often due to rotation. Even small degrees of rotation reduce the corrective effect. If the lens has rotated and the vault is appropriate, surgical rotation is usually the first step.
If a rotated lens is repositioned and remains stable, that often resolves the issue. If it rotates again, that suggests something about the anatomy does not support stable positioning. At that point, we reassess whether further intraocular intervention is appropriate. Repeated rotations are not a long-term strategy.
Lens Exchange
If the lens power is incorrect or vault is problematic, lens exchange may be considered. This means returning to the operating room and replacing the implant. While not technically complex, it is still intraocular surgery and carries the same categories of risk as the original procedure. It is reserved for situations where the visual benefit clearly justifies that additional risk.
Laser on Top of ICL
Surface laser enhancement (PRK or LASIK) can be performed after ICL in selected cases. I consider this when:
- The residual refractive error is small
- The cornea is suitable
- The patient prefers not to return to the operating room
Stacking procedures introduces cumulative risk. Even if small, it is not zero. Whenever possible, I prefer correcting the issue at the level of the ICL itself rather than adding a second refractive platform.
When to Stop
There is a point where additional intervention does more harm than good. If a patient does not see meaningful improvement with trial correction, further surgery is unlikely to transform the outcome. If a lens has already been rotated once and rotates again, repeating the same intervention is not wise.
Enhancement should produce real functional gain, not theoretical perfection. The goal is not 20/20 at any cost. The goal is 20-happy. If a patient is functioning well and comfortable, we do not chase tiny refractive numbers. Enhancement is a tool, not a reflex.
Eye Pressure, Dry Eye, and Secondary Issues Patients Miss
When patients think about ICL surgery, they focus on vision. What they often overlook are the secondary variables that influence outcomes just as much. Two in particular matter more than most people realize: intraocular pressure and ocular surface stability.
Eye Pressure: Why We Monitor It Closely
ICL surgery places a lens inside the eye. The lens is inserted through a small incision, then positioned behind the iris. Because of that, we are meticulous about monitoring intraocular pressure in the early post-operative period. Pressure is typically checked:
- Shortly after surgery
- The following day
- At structured follow-ups
Transient pressure elevations can occur. This may be related to retained viscoelastic material used during surgery or individual steroid response. In most cases, pressure normalizes quickly with medication if needed.
Sustained long-term pressure problems after modern ICL surgery are uncommon. However, early vigilance is essential. This is part of responsible intraocular surgery.
Dry Eye: The Hidden Amplifier
Many patients insist they do not have dry eye because they do not feel burning, irritation, or redness. That is not the full picture. A tear film can be unstable without obvious symptoms. Even subtle instability can amplify glare, ghosting, and visual fluctuation.
In some cases, what appears to be a lens-related complaint is actually ocular surface disease. This is why I optimize the corneal surface before surgery and continue managing it afterward. When the surface is stable, visual quality is more reliable.
Other Secondary Contributors
Persistent visual dissatisfaction is often attributed to the implant itself. But in many cases, contributing factors include:
- Residual refractive error
- Ocular surface instability
- Neural sensitivity
- Pupil dynamics
Inflammation is rarely a long-term issue when managed appropriately. The key is systematic evaluation rather than assumption.
The Clinical Approach
When a patient reports persistent symptoms, we do not jump to surgical revision. We first:
- Reassess refraction
- Evaluate tear film stability
- Recheck vault and lens position
- Confirm pressure is stable
Only after these variables are addressed do we consider further intervention.
ICL outcomes are not determined by the lens alone. They are influenced by measurement accuracy, surgical execution, pressure control, ocular surface health, and neuroadaptation. When these variables are managed carefully, most patients do extremely well. When patients understand these secondary factors, it prevents misattribution and unnecessary escalation of treatment.
ICL “Reversibility” Revisited: What Removal Really Means
One of the most attractive features of ICL surgery is that it is described as “reversible.” ICL can be removed or exchanged surgically. If the lens is removed and not replaced, the eye returns to its original refractive state. The myopia or astigmatism that was corrected by the implant returns.
From a structural standpoint, removal is generally straightforward. The lens often looks unchanged, even years later. However, removal still requires returning to the operating room. It is intraocular surgery again.
What Reversible Does Not Mean
Reversible does not mean temporary. It does not mean trying it for a few months and deciding later. It does not mean risk-free.
Each time we enter the eye, we reintroduce surgical risk — inflammation, pressure changes, endothelial considerations, and infection, however rare. For that reason, removal is not a convenience option. It is a contingency plan.
When Removal Is Considered
Removal or exchange may be considered when:
- Visual side effects are intolerable
- Vault is inappropriate
- Pressure cannot be controlled
- The lens power is clearly incorrect
In most cases, these decisions are made carefully and only after conservative options have been explored.
The Psychological Component
Some patients are reassured simply knowing the lens can be removed. It is important to understand that removal is another surgery, not a reset button. Reversibility is a safeguard, not a strategy.
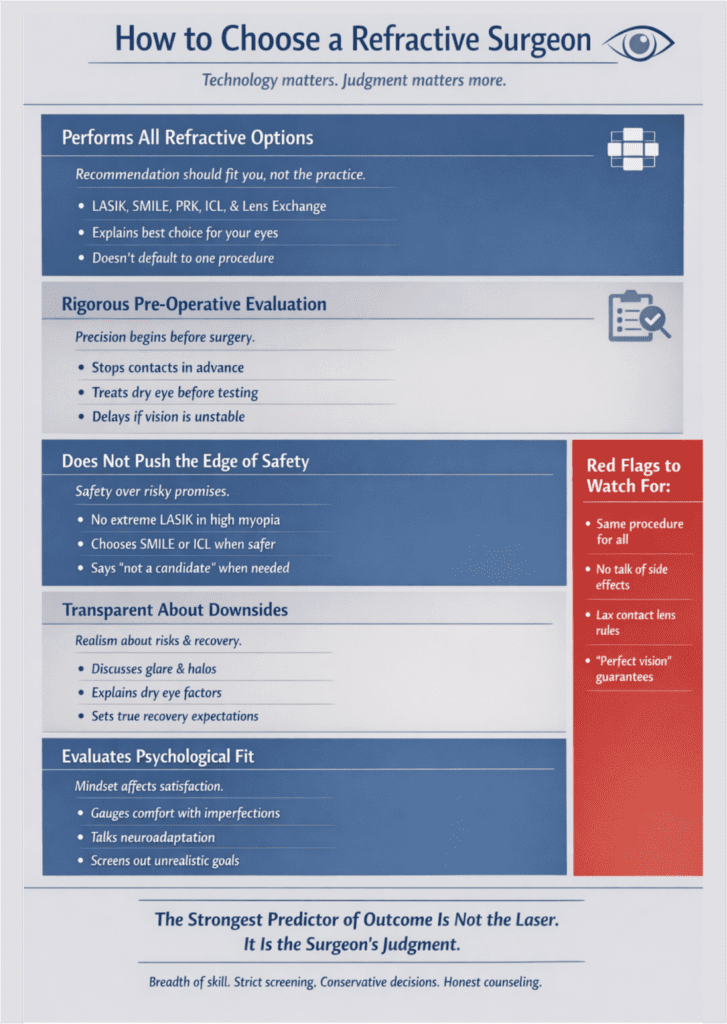
Choosing a Surgeon: Signals That Predict Outcomes
Patients often focus on technology. They ask which laser is used, which lens model is implanted, or which platform is newest. While important, these details are not the strongest predictors of outcomes. The eye surgeon matters more than the technology.
The best refractive surgeons are defined by the breadth of capability, strict screening standards, conservative risk tolerance, and honest counseling.
1. They Perform All Refractive Options
One of the most important signals is whether the surgeon performs the full range of refractive procedures: LASIK, SMILE, PRK, ICL, and refractive lens exchange. If a surgeon only performs one or two of these, their recommendations may be limited by what they offer.
When I evaluate a patient, I can recommend ICL, SMILE, LASIK, PRK, or lens-based surgery. The recommendation is based on what fits the patient — not what fits the practice.
2. They Are Strict About Pre-Operative Screening
Good refractive outcomes begin before surgery. An eye surgeon who is casual about contact lens discontinuation, dry eye optimization, refraction stability, and surface irregularity is increasing variability.
I am strict about these steps. If the measurements are not stable, I wait. If the surface is not optimized, we treat it first. Precision starts long before the operating room.
3. They Do Not Push Procedures at the Edge of Safety
A red flag is being pushed toward a procedure that sits at the edge of what is safe for your prescription. For example:
- Aggressive LASIK in very high myopia
- PRK when SMILE is clearly an option
- A recommendation that seems driven by what the surgeon performs most often
Patients should feel that the procedure was selected for them, not selected because it is the only tool available.
4. They Are Honest About Trade-Offs
A surgeon who minimizes glare, dry eye, or adaptation is not preparing you properly. Every refractive procedure has trade-offs. The goal is not to eliminate risk. It is to relocate it intelligently. If a surgeon explains both the benefits and the downsides clearly, that is a good sign.
5. They Filter for Expectations
Not every patient is a good refractive candidate, even if their eyes are technically suitable. Patients who expect perfection without adaptation, or who are unwilling to tolerate even small optical changes, may struggle regardless of the procedure. I do not operate on patients with unrealistic expectations. Surgical skill cannot compensate for a psychological mismatch.
The Reality
Refractive surgery outcomes are highly dependent on measurement accuracy, procedure selection, surgical execution, and post-operative management. All of those are human-dependent. Technology matters. Judgment matters more.
The Honest Value Proposition
ICL is a structural change in how your eye focuses light. When chosen appropriately, it can be life-changing. The patients who describe ICL as transformative are often:
- High myopes who have lived behind thick glasses for years
- Long-term contact lens wearers who are tired of daily dependence
- Patients who value preserving their cornea
- Highly active individuals who want stable, strong optics
For someone who is -8, -10, or higher, the visual freedom can feel dramatic. For these patients, ICL often provides clarity that would require significant corneal tissue removal with laser surgery.
What Patients Underestimate
The trade-offs are not usually about sharpness. They are about:
- Nighttime glare
- Neuroadaptation
- The patience required in the early months
- The responsibility of follow-up
Most patients adapt well. A small percentage require more time. A very small percentage require intervention. Understanding this before surgery changes how the experience feels afterward.
What I Tell Patients
If someone asks me to summarize ICL honestly, I explain it this way:
It is a custom-designed lens placed inside your eye to correct vision without removing corneal tissue. It offers excellent optical quality, particularly in higher prescriptions, and it preserves your natural cornea. It is removable, but it is still surgery inside the eye.
The Real Decision
The question is not whether ICL is better than LASIK, but whether:
- You are comfortable with intraocular surgery
- You value corneal preservation
- You understand the adaptation process
- You accept the different risk profile
When anatomy, expectations, and risk tolerance align, ICL can be one of the most rewarding procedures we perform. When they do not align, another procedure may be better.
The right answer is individualized.