Stye Surgery and Drainage: When It’s Appropriate and What Patients Should Know
Patients are often told they may need a stye surgery after days or weeks of discomfort, failed home treatments, or conflicting advice. The term itself can sound more serious than the procedure usually is, leaving many people unsure whether drainage is truly necessary, what it involves, or whether waiting could make things worse. This uncertainty is compounded by the fact that styes vary widely in how they behave and resolve.
This article explains when stye drainage is clinically appropriate, how doctors decide between observation, medication, and intervention, what the procedure actually feels like, and how recovery typically unfolds. The goal is to replace guesswork with clear decision logic, so patients understand not just what can be done, but why and when it makes sense.
Table of Contents
When a Stye Requires Surgical Drainage
Not every stye needs to be drained, and time alone is not the deciding factor. In clinical practice, the decision to intervene is driven far more by how the lesion behaves on exam than by how long it has been present.
The most important features clinicians assess are size, localization, and fluctuation. A stye that feels soft, round, and fluctuant, similar to a small abscess, is often a good candidate for drainage. These lesions tend to be active and localized, making them easier to decompress. In contrast, older styes that have become firm or scarred are often harder to drain and may not respond as completely.
Contrary to common assumptions, earlier, more active styes are sometimes easier to drain than older ones. Early lesions are more likely to be fluid-filled and less fibrotic. Once scarring sets in and the lesion transitions toward a chalazion, drainage becomes less predictable.
Pain level is not a reliable guide. Most styes are uncomfortable regardless of whether drainage is appropriate. While larger or deeper lesions can cause more irritation, pain alone does not determine whether intervention is needed.
Functional impact does matter. If a stye distorts the eyelid, presses on the cornea, interferes with vision, or affects daily activities, clinicians may recommend earlier intervention. Cosmetic timing can also be a legitimate consideration, particularly when a visible lesion is not improving and matters to the patient.
Importantly, there is no fixed timeline that applies to every case. Some styes are drained the same day they are evaluated. Others are safely observed for weeks if symptoms are tolerable and the lesion is evolving. In most cases, styes are not dangerous and do not threaten long-term vision. The decision to drain is individualized, balancing physical findings with patient tolerance and expectations.
The factors below summarize how clinicians weigh whether drainage is appropriate, recognizing that no single factor applies in isolation.
| Clinical Factor | What Doctors Look For | How It Influences Drainage Decisions |
| Size and bulk | Larger, rounder lesions | Larger styes are more likely to be drained, especially if well-defined |
| Fluctuation | Soft, fluid-filled, abscess-like feel | Strong indicator that drainage will be effective |
| Localization | Clearly confined to one area of the lid | Localized lesions are easier and safer to drain |
| Scar formation | Firm, fibrotic, non-compressible tissue | Scarred lesions are harder to drain and may respond less completely |
| Timing | Acute vs long-standing | Early, active styes are often easier to drain than older ones |
| Pain level | Discomfort or pressure | Pain alone does not determine the need for drainage |
| Vision interference | Lid distortion or corneal pressure | Functional impact may justify earlier intervention |
| Cosmetic or practical impact | Visibility, upcoming events, daily disruption | Patient priorities can reasonably influence timing |
| Response to home care | Failure of warm compresses or drops | Lack of improvement supports considering drainage |
| Patient tolerance | Willingness to wait vs intervene | Individual tolerance plays a legitimate role |
How Doctors Decide Between Observation, Medication, and Drainage
When a patient presents with a stye, the first step is to decide whether intervention is needed at all. Many styes improve without procedures, and early management focuses on reducing inflammation and supporting natural resolution.
Clinically, most styes are primarily inflammatory, not purely infectious. They originate from blockage and inflammation of the eyelid’s oil glands, often in the setting of underlying blepharitis or meibomian gland dysfunction. Bacteria may be present, but infection is rarely the sole driver. This is why antibiotic-only treatment often fails.
Early treatment typically includes topical steroid–antibiotic combinations, rather than antibiotics alone. The steroid component addresses inflammation within the gland, while the antibiotic reduces secondary bacterial overgrowth. Patients who have only received antibiotic ointments frequently see limited improvement until inflammation is treated directly.
Observation remains appropriate when a stye is small, early, and tolerable. In these cases, topical therapy, eyelid hygiene, and compresses are often sufficient. Drainage may be delayed if the lesion is too small to localize safely, as premature excision can increase scarring without fully resolving the problem.
Oral antibiotics are not routine for uncomplicated styes. They are reserved for specific situations, most notably when there are signs of preseptal cellulitis, where redness, swelling, and tenderness extend beyond the localized lesion into the surrounding eyelid tissue. In these cases, oral antibiotics are used to control the broader infection, not to treat the stye itself.
More serious findings, such as pain with eye movement, double vision, marked eye redness, or rapidly worsening swelling, raise concern for orbital cellulitis, a rare but urgent condition. These patients require immediate evaluation and often intravenous antibiotics. This escalation is driven by the spread of infection, not by the stye alone.
Drainage becomes the preferred option when conservative treatment fails or when the lesion has formed a localized abscess. In these cases, medication alone may reduce inflammation but cannot evacuate trapped material. Drainage is often combined with continued topical therapy to support healing and reduce recurrence.
Patient-specific factors also influence decision-making. Children, highly anxious patients, or individuals with bleeding disorders may not be ideal candidates for immediate drainage. In contrast, patients experiencing significant functional impairment or ongoing progression despite appropriate treatment may benefit from earlier intervention.
A common misunderstanding is that drainage represents “surgery.” In reality, stye drainage is an in-office procedure performed under local anesthesia. It is one step within a broader treatment sequence, not a failure of conservative care. When used at the appropriate stage, it can shorten symptoms and reduce frustration without increasing risk.
What Happens During Stye Drainage
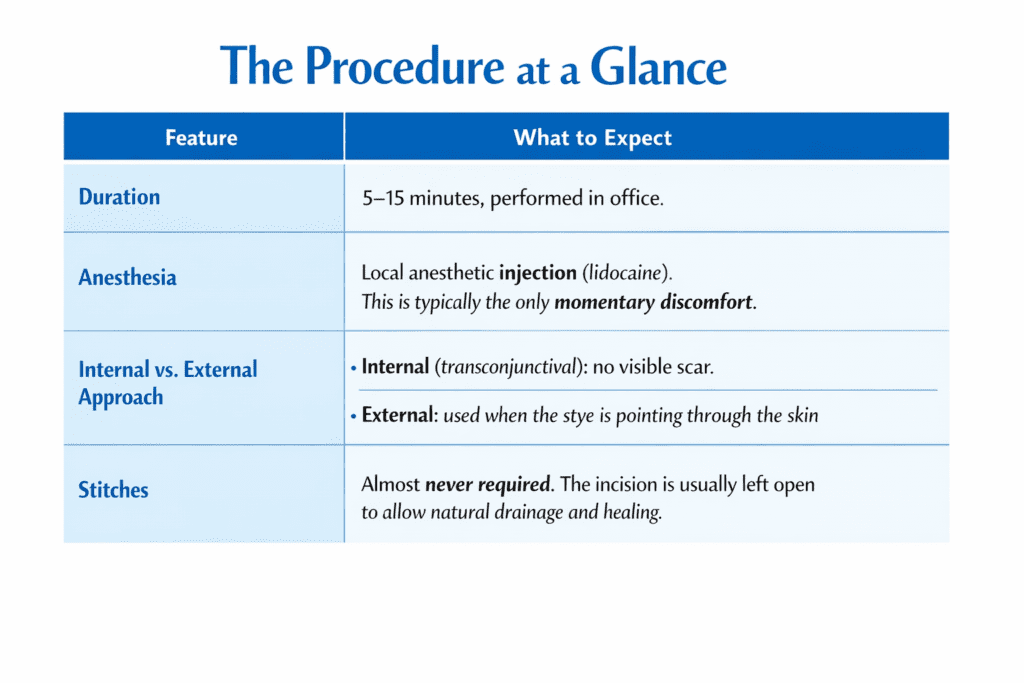
Stye drainage is a brief, in-office procedure. It does not require an operating room, general anesthesia, or hospital admission. From start to finish, it typically takes five to fifteen minutes.
The steps below outline what typically happens, in the order patients experience it.
- Preparation and Positioning: The eyelid is cleaned, and the patient is positioned comfortably, usually in a reclined chair. The eye itself is protected throughout the procedure.
- Local Anesthesia: The eyelid is numbed with a local anesthetic injection. Numbing creams are avoided because they can irritate the surface of the eye. The anesthetic often includes epinephrine to reduce bleeding and bruising. The injection causes a brief burning sensation that lasts a few seconds. Once numb, patients feel pressure and touch but no sharp pain.
- Confirming Numbness: Before making any incision, the clinician confirms that the eyelid is fully numb. The procedure does not proceed until adequate anesthesia is achieved.
- Incision Placement: The incision location depends on where the stye is located. External styes are incised from the outside of the eyelid, while Internal styes are approached by gently flipping the eyelid and incising from the inside. This decision is based on access and anatomy, not cosmetic preference.
- Drainage of the Stye: A small, controlled incision, usually two to four millimeters, is made. The contents of the stye are expressed using gentle pressure and specialized sterile instruments. Some bleeding is expected and not concerning. Cautery is not used.
- Healing Approach: Stitches are not required. The incision is left open to heal naturally. A steroid-antibiotic ointment is applied, and in some cases, a temporary patch is placed.
- Post-procedure Check: Before the patient leaves, the clinician confirms that the lesion has decompressed and reviews aftercare instructions.
Patients remain awake and communicative throughout the procedure and can pause or reposition at any time.
Pain, Anesthesia, and What Patients Feel
Fear of pain is one of the main reasons patients hesitate to proceed with stye drainage. In practice, discomfort is limited and predictable, and most patients tolerate the procedure better than they expect.
The only part of the procedure that is typically painful is the local anesthetic injection. The lidocaine causes a brief burning sensation that lasts a few seconds. Once the anesthetic takes effect, sharp pain is eliminated. Patients describe feeling pressure, movement, or touch, but not cutting or piercing sensations.
During drainage itself, discomfort comes mainly from pressure applied to express the contents of the stye. This can feel intense for a moment, particularly if the lesion is large, but it is not experienced as pain in the usual sense. The sensation is temporary and ends as soon as the pressure stops.
Patients remain fully awake throughout the procedure and can communicate at any time. If a patient feels uncomfortable or needs a pause, the procedure can be slowed or repositioned.
This sense of control is often reassuring for people who are anxious about eye procedures.
For patients with significant anxiety, additional steps can help. Some are prescribed a mild oral anti-anxiety medication before the appointment. Others benefit from distraction techniques, such as holding a stress ball or using vibration-based tools designed to reduce procedural awareness. These measures are optional and tailored to the individual.
In the first 24 hours after drainage, mild soreness, swelling, and tearing are normal. Post-procedure discomfort is usually less than the pain caused by the untreated stye. Worsening pain, increasing redness, or progressive swelling are not expected and should prompt follow-up.
There is no meaningful difference in pain experience between drainage of an acute stye and a chalazion. What varies most is individual tolerance for the anesthetic injection and for procedures involving the eye, rather than the procedure itself.
Recovery Timeline, Aftercare, and Cosmetic Outcomes
Recovery after stye drainage is usually straightforward and faster than patients expect. Most people resume normal activities the same day.
Immediately after the procedure, mild swelling, redness, or tenderness of the eyelid is common. This typically improves over the first 24 to 48 hours. Bruising can occur, but is uncommon when the procedure is performed on an active, localized lesion.
Aftercare focuses on inflammation control and hygiene. Patients are advised to continue prescribed drops or ointments, usually a steroid–antibiotic combination. Keeping the eyelids clean is important during healing. Warm compresses may be continued if recommended, but excessive heat or irritation should be avoided.
Downtime is minimal. Patients can return to work, screens, and light exercise the same day. Contact lenses and eye makeup should be avoided for a few days to reduce irritation and reinfection risk. If makeup is necessary for work, it should be removed promptly, followed by proper lid hygiene.
Cosmetic outcomes are generally favorable. Incisions are small and placed to minimize visibility. Stitches are not used, and the eyelid heals naturally. In selected cases, clinicians may use anti-scarring injections to further reduce the risk of visible marks or lid irregularities.
Timing matters. Earlier drainage of active, fluid-filled styes often leads to faster resolution and better cosmetic results. Older, scarred lesions may flatten more gradually and may not resolve completely after a single procedure.
Patients should contact their doctor if swelling, redness, or tenderness worsens instead of improving, or if new symptoms develop. Follow-up is typically straightforward and focused on confirming resolution and addressing underlying eyelid conditions to reduce recurrence.
Risks, Complications, and When Drainage Is Not Enough
Stye drainage is generally low risk when performed at the appropriate stage, but no procedure is risk-free. Understanding what is common, what is uncommon, and what is concerning helps make informed decisions and respond appropriately after treatment.
The most common issues after drainage are minor and temporary. These include mild bleeding during the procedure, short-term swelling, and tenderness. In some cases, the stye improves but does not flatten completely. This usually reflects underlying scarring or a transition toward a chalazion rather than a procedural failure.
Recurrence is possible. Some patients develop repeated styes because the underlying eyelid condition has not been addressed. Drainage treats the active lesion, but it does not correct blepharitis or meibomian gland dysfunction. Ongoing eyelid care is essential to reduce future episodes.
More serious complications are uncommon but important to recognize. Infection, significant bleeding, or worsening inflammation after drainage are not expected. Rarely, aggressive or poorly timed drainage can worsen scarring or cosmetic outcomes, which is why not every stye should be drained.
Certain patients carry a higher risk. Those with bleeding disorders, on blood-thinning medications, with compromised immune systems, or with poorly controlled diabetes may require additional precautions or alternative timing.
Persistent or atypical lesions require further evaluation. If a bump does not respond as expected, recurs in the same location, or has unusual features, additional treatment or investigation may be needed to rule out non-stye causes.
After Stye Drainage: What’s Normal vs When to Seek Care
| Situation | What This Usually Means | Recommended Action |
| Mild swelling or soreness for 1–2 days | Normal post-procedure inflammation | Monitor; continue prescribed aftercare |
| Light bleeding during or shortly after the procedure | Expected with active lesions | No action unless bleeding persists |
| Lesion improves but does not fully flatten | Residual scar or chalazion tissue | Observation or follow-up if bothersome |
| Stye recurs in the same area | Underlying eyelid disease | Address blepharitis or gland dysfunction |
| Increasing redness spreading beyond the stye | Possible infection | Contact provider promptly |
| Worsening pain after initial improvement | Not typical | Seek re-evaluation |
| Fever or systemic symptoms | Possible spreading infection | Urgent medical assessment |
| Double vision or eye movement pain | Possible orbital involvement | Immediate evaluation |
| Repeated non-resolving lesion | Atypical process | Further investigation may be needed |
Drainage is most effective when used selectively, not reflexively. When recovery does not follow the expected course, early reassessment is safer than waiting. Most complications are avoidable with proper timing, technique, and follow-up.
In Summary
Stye drainage is not a default step or a failure of conservative care. It is one option within a broader treatment sequence, used when exam findings, symptom progression, and patient tolerance align. Most styes are not dangerous, but delaying appropriate treatment can prolong discomfort and complicate recovery. Clear evaluation, proper timing, and attention to underlying eyelid health are what ultimately determine outcomes, not the procedure alone.
Frequently Asked Questions About Stye Drainage
Does a stye always need to be drained?
No. Many styes improve with medication and eyelid care alone. Drainage is considered when a stye forms a localized abscess, persists despite treatment, or causes functional or cosmetic problems.
How do doctors decide whether to drain a stye or wait?
The decision is based on exam findings such as size, fluctuation, and localization, not just how long the stye has been present. Patient tolerance and daily impact also factor into timing.
Is stye drainage painful?
The anesthetic injection causes brief burning for a few seconds. After that, patients feel pressure but not sharp pain during the procedure.
Will draining a stye leave a scar?
Scarring is uncommon when drainage is done appropriately. Incisions are small, carefully placed, and heal naturally. Anti-scarring measures may be used when indicated.
When should I seek urgent care instead of waiting?
Immediate evaluation is needed for rapidly worsening swelling, spreading redness, fever, double vision, pain with eye movement, or vision changes.